
Why the Hoof Wall Lies
Capsule Divergence, the Persian Slipper, and What It Means for Your Horse
Caldwell & Madden · Scientific Horseshoeing Limited · hoofflix.com
Based on the biomechanical framework set out in The Equine Foot (Caldwell & Madden, 2025) and the F9 therapeutic farriery protocol of O’Grady & Steward (AAEP 2007/2009). Trimming protocol and illustrations: Dr Stephen E. O’Grady DVM MRCVS · Virginia Therapeutic Farriery · equipodiatry.com
Who this article is for |
This article is written for horse owners, yard managers, and semi-professional hoof care practitioners. It uses plain English throughout. Technical terms are introduced and explained as they arise. No prior knowledge of anatomy or biomechanics is assumed. |
The question most people never think to ask
When a horse develops laminitis and the hoof begins to change shape, most people talk about “rotation.” The pedal bone has rotated. The radiograph shows the angle. A number is given — six degrees, twelve degrees, eighteen degrees — and that number becomes the measure of how bad things are.
why does the outside of the hoof wall stop following the bone?
Understanding the answer changes the way you read a radiograph, changes the way you look at a hoof on the ground, and changes the way you understand what the farrier or vet is trying to achieve. It also changes what the prognosis figures mean — and that matters enormously when you are making decisions about a horse you care about.
This article explains the physics of what happens to the hoof wall and the sole when the lamellar connection fails, why the classic “Persian slipper” or “ski-jump toe” develops even when the pedal bone has barely moved at all, and why a horse can lose critical sole depth without any radiographic joint deviation. It then explains how a hidden second mechanism compounds the situation in ways that traditional rotation grading does not capture.
Part One: How horn grows
The hoof wall is not a rigid tube
The hoof wall is produced continuously at the coronary band — the band of tissue that runs around the top of the hoof like a hairline. New horn is laid down there every day, at a rate of roughly five to ten millimeters per month. This new horn then slides downward, carried along by the continuing production of more horn above it, until it reaches the ground.
The hoof wall is therefore not a fixed structure. It is a slow-moving sheet of horn, permanently in transit from the coronary band to the ground. At any given moment, the piece of wall you can see near the toe has been travelling for roughly a year. The piece at the heel may only have been growing for four or five months.
D’Arcy Wentworth Thompson — On Growth and Form (1917) |
Thompson showed that biological structures are not simply static objects — they are the visible record of the forces acting on growing material over time. A shell, a bone, a hoof wall: each one is a frozen history of growth. The shape of the structure tells you what forces were present when it was being formed. |
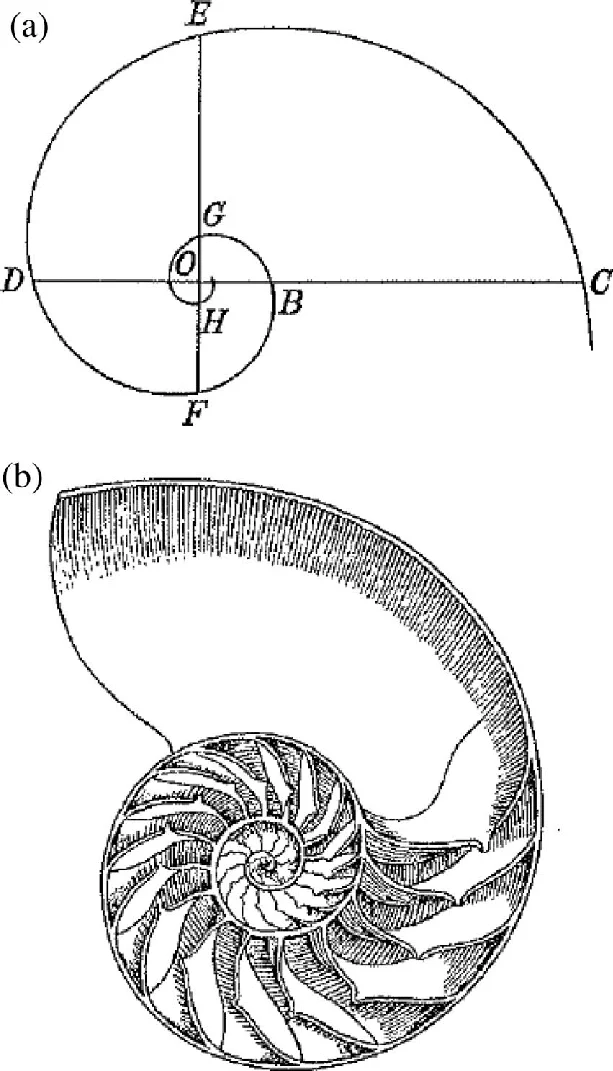
The spiraling logarithmic curve of horn growth (Darcy Wentworth Thompson 1917)
In a healthy horse, the hoof wall grows downward from the coronary band whilst remaining in close contact with the underlying pedal bone (P3). The outer surface of the pedal bone is covered with tiny interlocking projections — the primary and secondary dermal lamellae — which bond to corresponding lamellae on the inside of the hoof wall. This bond holds wall and bone together as the wall grows, so the wall follows the bone’s angle precisely.
The dorsal hoof wall angle (DHWA) — the angle the front face of the hoof makes with the ground — is therefore a near-perfect reflection of the angle of P3’s own front face. In a healthy foot, those two angles are almost identical.
The wall follows the bone.
Part Two: What happens when the lamellar bond fails
Laminitis is, at its root, a failure of this bond. The lamellae become inflamed, the blood supply to the lamellar tissue is disrupted, and the microscopic interlocking projections that hold wall to bone begin to break down. The lamellar connection weakens.
At this point, a mechanical competition begins. On one side: the weight of the horse pressing down through the skeleton. On the other side: the increasingly fragile lamellar tissue holding the bone away from the ground.
As long as the lamellae hold, the bone stays where it is and the wall follows the bone. But if the lamellae fail even partially — particularly at the toe, where the load is highest — a gap begins to open between the bone and the wall. New horn continues to be produced at the coronary band. It slides downward. But now, instead of growing along the face of the bone, it grows into space. The wall and the bone are no longer coupled.
Divergence — the key word |
Divergence means the uncoupling of wall from bone. Not simply rotation — though rotation may come later — but the separation of two structures that should be moving together. The wall begins its own independent journey downward, no longer following P3’s parietal surface. |
Part Three: The geometry of divergence
Why the toe grows long — but not in the way you might think
When the dorsal lamellae fail, the wall at the toe stops following the bone. The bone may remain in its correct position relative to the ground — no radiographic rotation yet. But the wall keeps growing. And because it is no longer tracking the bone, the angle the wall makes with the ground decreases. The toe slopes forward and downward more and more shallowly.
This is the “long toe” of laminitis. But it is not a long toe in the way a neglected sound horse gets a long toe:

laminal wedge highlighted by the white lines and arrow and the divergent hoof wall, normal orientation on the left.
Two completely different mechanisms — same appearance from the outside |
Neglected sound horse: the wall grows more than usual; the toe increases in length but still follows the bone. The angle is roughly maintained. The structure is normal, just overgrown. Laminitic horse: the wall has stopped following the bone and grows in a progressively different direction. The front face of the wall diverges away from the front face of P3. The space between them fills with a weaker horn-like material — the lamellar wedge — which is visible on a radiograph as a grey zone between the two bright white structures. |
Why the sole thins — even without measurable rotation
Now consider what happens to the sole. The sole is produced by tissue on the bottom of the pedal bone. It grows downward to form the concave surface under the foot. The thickness of the sole at any given point is the distance between the solar surface of P3 and the outer bearing surface of the sole horn.
As the wall diverges and the lamellar wedge thickens at the toe, the white line — the junction between wall horn and sole horn — migrates inward and upward. The solar horn at the toe, which was once relatively thick, is progressively stretched thin as the wall pulls away from it. The sole at the toe becomes the material that bridges the gap between the grounded bearing surface and the now-lower P3 solar surface. It stretches. It thins.
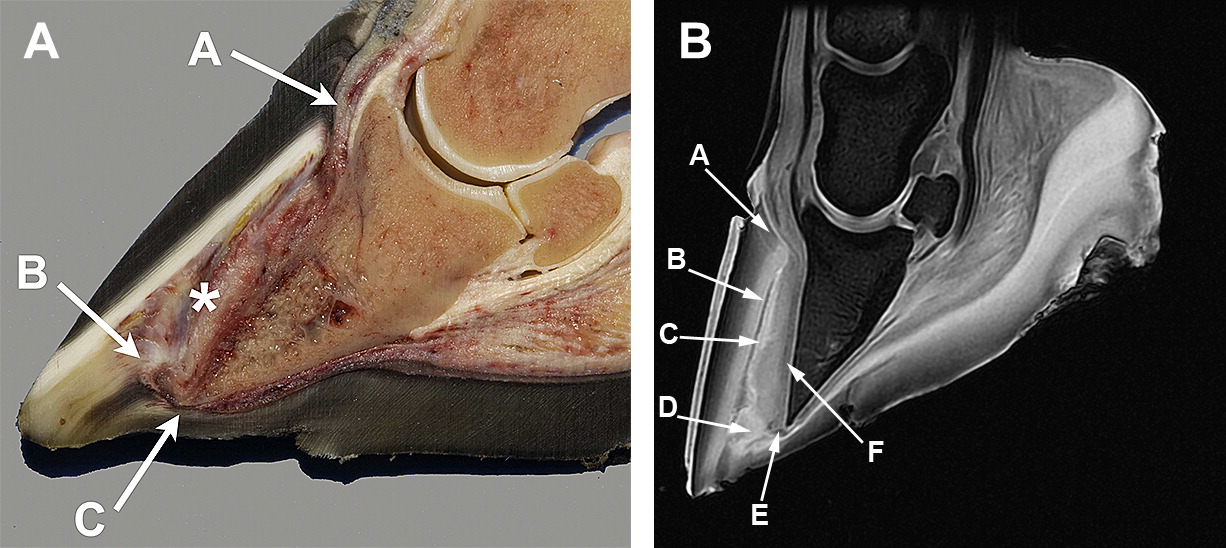
left A) coronary band, B)terminal papillae , compressed solar corium.
right A) coronary papillae B) epidermal lamellar C) distended dermal lamellar D) lamellar wedge E) vascular F) lamellar corium
Critical clinical point — sole thinning precedes measurable rotation |
This thinning occurs even when no axial rotation of P3 has yet been measured on a radiograph. The bone may still be sitting at a perfectly normal angle. The radiograph may show no DIPJ deviation at all. But the sole is already thinner than it was because the wall has moved away from the bone and the sole horn is being drawn out to fill the growing space. Waiting for a rotation figure before worrying about sole depth can mean the horse is already in trouble that the radiograph has not yet caught up with. |
Part Four: The Persian Slipper
A growth form governed by physics
D’Arcy Wentworth Thompson would have recognised the Persian slipper hoof immediately as a classic example of differential growth producing a predictable form.
In a foot with established lamellar divergence, the coronary band at the toe begins to drop. This happens because the lamellar wedge — which is structurally weaker than normal hoof wall — no longer supports the skin above it in the same way. The coronary band sinks and migrates slightly forward. The new horn produced at this dropped coronary band grows downward and forward at a progressively shallower angle. The resulting shape is a wall that curves upward and outward at the toe.
The physics are straightforward. Growth at the coronary band proceeds in the direction the coronary band is pointing. If the coronary band is tilted forward, growth proceeds forward and down. If the growing tube of wall is being pushed forward by the expanding lamellar wedge, the wall curves progressively forward with each new layer of horn added above. The final form is not an accident.
What you can read in the hoof — without a radiograph |
- A dipped or stepped coronary band at the toe indicates the lamellae have failed there and the coronary band has dropped
- A flattened or reversed hoof wall angle indicates advanced divergence
- Growth rings that are wider at the heel than the toe indicate that heel growth has continued normally whilst toe growth has slowed or stopped — a classic laminitis marker
- A sole that feels thin, flat, or ‘dropped’ to the examiner’s thumb indicates that the P3 solar surface is approaching the ground


gross dorsal migration of the DHW resulting in loss of vertical height stretching of the white line stretching and thinning of the sole and a subsequent loss sole depth
Part Five: The two mechanisms of rotation — and why one is invisible
Traditional rotation grading measures a single angle: the angle between the front face of P3 and the front face of the hoof wall, as seen on a calibrated lateral radiograph. This is a perfectly valid measurement. But it only captures one of two quite different mechanisms by which the loading geometry of the foot changes.
Mechanism 1: Lamellar rotation
The pedal bone rotates within the hoof capsule as the lamellar bond fails. P3 tips so that its toe points toward the ground. This is what the rotation angle on the radiograph shows. The horse’s toe-to-heel alignment at the DIPJ (the coffin joint) may remain normal — the joint itself has not deviated. It is purely a lamellar failure.
Mechanism 2: Flexural deformation at the P2–P3 joint
In a healthy horse, the pastern bone (P2) and the pedal bone (P3) meet at an angle of approximately three to five degrees. The solar surface of P3 faces very slightly backward and downward. This is the normal palmar angle.
When the deep digital flexor tendon (DDFT) is under sustained high tension — as it is in laminitis, where the rotation mechanism described above dramatically increases the mechanical demand — the P2–P3 joint can be progressively loaded into hyperextension. P3 tilts further backward, so that its solar surface faces more and more palmarly. The palmar angle increases beyond the normal three to five degrees.
This is a joint change, not a lamellar change. It is independent of whether the wall has rotated relative to the bone. A horse can have a large palmar angle with very little radiographic wall-to-bone rotation, or it can have both present simultaneously.
The compound correction angle
When both mechanisms are present, their effects on DDFT tension are additive. The effective correction angle is not simply the lamellar rotation figure:
Effective correction angle = lamellar rotation° + the amount by which palmar angle exceeds 5° |
If a horse has eight degrees of lamellar rotation and a palmar angle of nine degrees, the excess palmar angle is four degrees, and the effective correction angle is twelve degrees — half as severe again as the rotation figure alone would suggest. The prescription for heel elevation, the force on the lamellar tissue at each stride, and the clinical prognosis are all materially different.
Clinical signs that suggest the palmar angle component is present — O’Grady (2007) |
The horse lands toe-first when walking. It becomes lame shortly after trimming. When you ask it to move a foreleg backward, the heel fails to contact the ground. Each of these indicates that the DDFT is under shortening tension that is not being adequately accounted for by the rotation figure alone. |
Part Six: Founder distance, sole depth, and prognosis
The radiograph gives us two numbers that are particularly useful for assessing severity and predicting outcome.
Sole depth
Sole depth is the distance from the solar surface of P3 to the outer bearing surface of the sole horn. Normal is fifteen millimetres or more. Below twelve millimetres, the horse is at genuine risk of P3 penetrating through the sole. Below eight millimetres, that risk is immediate. As explained in Part Three, the sole thins because the wall has diverged from the bone and the sole horn has been stretched to fill the growing gap.
Founder distance
Founder distance measures how far P3 has displaced downward within the hoof capsule — not just the rotation, but the absolute sinking. In a Thoroughbred, the normal figure is approximately five millimetres. Above eleven and a half millimetres, the prognosis worsens significantly. Above fifteen millimetres, the horse is almost certainly in the distal displacement (sinking) category — a condition with a fundamentally different and much more guarded prognosis.
Published prognosis figures (Cripps & Eustace 1999; French et al. 2007)
Condition | Return to previous use | Survival | |
| Rotation <11.3° · no sinking | ~83% | ~72% | Cripps & Eustace 1999 |
| Rotation ≥11.3° · no sinking | ~57% | ~65% | Cripps & Eustace 1999 |
| Any distal displacement (sinking) | ~27% | ~44% | Cripps 1999; French 2007 |
| Bilateral sinking | ~11% | — | Cripps & Eustace 1999 |
| Sole penetration by P3 | ~5% | ~22% | Cripps 1999; French 2007 |
The compound rotation caveat |
These figures assume that the rotation measurement alone captures the severity of the condition. They were collected before the compound rotation model — incorporating the palmar angle component — was widely recognised as a separate and additional factor. A horse with eight degrees of lamellar rotation and a palmar angle of nine degrees is not clinically equivalent to a horse with eight degrees of rotation and a normal palmar angle. The former is under more DDFT load at every stride. The prognosis, though not yet captured by published figures, should be considered more guarded than the rotation grade alone would indicate. |
In practical terms: if your horse has a borderline rotation figure but is landing toe-first, is lame after trimming, or is showing a rapidly increasing founder distance on sequential radiographs, do not assume that the rotation number tells the full story. Ask your vet and farrier about the palmar angle, and whether the heel elevation being prescribed is based on the effective correction angle or the lamellar rotation figure alone.
Part Seven: What good trimming and shoeing is trying to achieve
Given all of the above, the logic of the trimming and therapeutic shoeing protocol used in serious laminitis cases becomes much clearer.
Step 1 — Bearing surface trim (Savoldi)
The heel is set at approximately frog height. The heel setback from the bulb is typically about fourteen per cent of the foot’s sagittal length — approximately eighteen millimetres on a 130mm foot. Nothing is removed from the solar surface toward the toe: the sole there is already compromised and every millimetre is protecting P3. The frog is trimmed only to its natural divergence point. The white line is cleaned out so the farrier can see exactly where to position the shoe.
Step 2 — The dorsal wall rasp
The object of this rasping is not to produce a cosmetically normal hoof angle. It is to restore, as far as possible, the approximate parallel alignment between the external wall surface and the parietal surface of P3 — to restore wall–P3 parallelism.
| Target wall angle = current DHWA° − rotation° (P3 parietal surface angle) |
At eight degrees of rotation and a DHWA of forty-four degrees, the target external wall angle is thirty-six degrees — not fifty. Rasping toward fifty on this foot would actively worsen the divergence. Sole depth gates this work absolutely: below twelve millimetres any wall reduction near the ground surface is dangerous, and below eight millimetres the dorsal rasp is stopped entirely.
Step 3 — Heel elevation
Applied after the trim in most cases — unless the horse is showing signs of DDFT shortening, in which case elevation is applied before trimming to protect against the lameness that can result from reducing the foot without first releasing the tendon tension.
| Elevation = sagittal length × sin(effective correction angle°) |
The shoe is then positioned precisely to the CoR datum — the centre of rotation of the coffin joint. Breakover is set approximately twenty-two millimetres palmar to the apex of P3. Palmar support fills the palmar two-thirds of the sole, transferring load from the damaged lamellar tissue to the healthier digital cushion. The dorsal toe region is always left clear: applying support material under P3’s apex when the sole is thin would cause direct pressure on the already-compromised lamellae.
In summary: what every owner and practitioner should know
- The hoof wall is not rigidly attached to the pedal bone. It is held there by a continuous biological bond — the lamellae — that must be maintained by a healthy blood supply and intact lamellar tissue.
- When this bond fails at the toe, the wall and the bone diverge. The wall continues growing downward; the bone no longer guides it. This is capsule divergence. It produces the Persian slipper form because horn growth at the dropped coronary band proceeds in the direction the coronary band is pointing.
- The sole thins during divergence even without measurable rotation. The stretching of the white line and solar horn at the toe reduces sole depth before the bone has measurably tilted. Sole depth on a radiograph should always be taken seriously, irrespective of the rotation figure.
- Rotation measures the angle between wall and bone at the time of the radiograph. It is a useful measurement but it does not capture the full clinical severity when a palmar angle component is also present.
- The effective correction angle is lamellar rotation plus excess palmar angle. This is the number that governs DDFT load, treatment requirements, and, likely, prognosis.
- Founder distance measures total downward displacement of P3. Rising founder distance on sequential radiographs, combined with increasing palmar angle, suggests the disease is progressing in ways that the rotation figure alone does not reveal.
- Good trimming restores wall–bone geometry. Good shoeing decompresses the DDFT. These are not cosmetic interventions. They are mechanical corrections applied to specific mechanical problems. Understanding the physics helps you understand why both are necessary, why sequence matters, and why partial implementation is not as good as doing it properly.
References & Further Reading
- Caldwell A., Madden J. (2025). The Equine Foot: Science, Craft and Clinical Reasoning in Farriery and Podiatry. Scientific Horseshoeing Limited. [Compound PA model, CoR-referenced shoe placement, dual-vector ML model]
- Cripps P.J., Eustace R.A. (1999). Factors involved in the prognosis of equine laminitis in the UK. Equine Vet J 31(5):427–432.
- French K.R. et al. (2007). Survival and return to use data in chronic laminitis. Cited in Caldwell & Madden 2025.
- O’Grady S.E., Steward M.L. (2007). The wooden shoe as a therapeutic device. Proceedings AAEP 2007.
- O’Grady S.E. (2009). Therapeutic farriery for laminitis: the wooden shoe. Equine Vet Educ 21(8):419–426.
- O’Grady S.E. (2007). Clinical indicators of DDFT shortening. AAEP Proceedings. [Toe-first landing, lame after trim, heel non-contact]
- Thompson D’A.W. (1917). On Growth and Form. Cambridge University Press. [Biological structures as records of growth forces]
- Pollitt C.C. (various). Lamellar physiology, blood flow, and penetration risk thresholds.
- Redden R.F. (various). Sole depth reference values and rim pad thresholds in laminitis management.
- Meier A., Schramme M.C., Hunter B. (2019). Modified Obel grading system for equine laminitis. PeerJ 7:e7084.