
What “The Toe Is Not a Lever” Isn’t Telling You About Your Horse
A viral post is telling owners that toe length doesn’t matter for laminitic horses, and that the vets and farriers recommending you take the toe back are wrong. The published research, the radiographs, and the case histories say something very different. Your horse can’t tell you which side is right. So here it is, plainly
Open source response by the HoofFlix team. Mark Caldwell Ph.D. FWCF., Neil Madden FWCF., & Sam Fowler Dip. WCF.
The Facebook post at the centre of this is doing something most online hoof-care arguments don’t. It’s reaching for first principles. It uses engineering vocabulary correctly. It cites measured ground reaction forces and material properties. It works through actual calculations. That’s rare in this corner of the internet, and it isn’t the problem.
The problem is that all of that careful structural reasoning has been applied to the wrong mechanical system. This article uses the same framework, the same kind of measurements, the same engineering logic, to show where the post goes wrong, why your horse pays the price for it, and what you should be asking for instead.
A quick note on sourcing before we start. Some of what this article responds to comes directly from the original post: the lever claim, the 0.2 mm calculation, the description of how the leg moves at the end of stance. Other arguments come from comments, replies, and the wider rehabilitation method that has grown up around the post: the framing of the lamellar wedge as “the toe wall,” the “three points of support” claim, the idea that previous corrective trimming caused the distortion in the first place. The post and the protocol it has become attached to are not quite the same thing, and it’s worth knowing which is which.
If you’ve watched a horse struggle with laminitis, you already know the feeling.
The bounding pulses you didn’t notice the day before. The way they suddenly don’t want to walk. The vet on the phone, the farrier on the way, the radiographs you didn’t really understand. The waiting. The wondering whether you missed something. The long, slow growing-out of a hoof.
And if you’ve then watched conventional treatment fail, or watched your horse get progressively lamer under farriery you trusted and paid for, you’d be ready to listen to anyone who said there was a better way.
That’s the territory a particular online community has built itself in. The promise is appealing. A kinder, more natural method. Don’t take the toe back. Drop the heels. Let the foot grow at its own pace. Trust the horse. Distrust the professionals who got you to this point.
And the technical-sounding argument that ties it all together is this: the toe of the equine hoof is not a lever. There is a long, eloquent Facebook post making the engineering case. The maths is shown. The deflection of the hoof wall under load is calculated. The conclusion is firm. Toe length doesn’t generate harmful forces. Anyone telling you otherwise is wrong.
It’s a compelling argument. And in places, it’s genuinely right.
Here’s what they have right. The hoof wall really doesn’t bend much under load. The maths in that post is sound: the capsule is a curved, continuous, internally reinforced structure, and a force pushing on it from the ground would barely move it. The 0.2 mm deflection they calculate is about right. They’re also right about something bigger. Conventional farriery has failed an enormous number of laminitic horses. Long-toe low-heel farriery (leaving toes too long for too long, shoeing cycle after shoeing cycle) is one of the main reasons we end up with the distorted feet they’re now trying to rehab. And they’re right that dropping the heels and letting new, properly attached hoof wall grow down from the coronary band is part of what real rehabilitation looks like. That much is sound.
Here’s where the wheels come off. The toe IS a lever. Just not the lever the post tried to disprove. The lever isn’t the wall bending; it’s the long arm that a long toe creates between the ground and the joint inside the foot, every single time your horse pushes off. Researchers using force plates have shown that a 10 mm shift in breakover reduces peak deep flexor tendon tension by about 21 per cent.¹,² That tendon runs across the back of your horse’s navicular bone. Over ten thousand strides a day, the difference is enormous. And the long “toe” the protocol is telling you to preserve isn’t a structural pillar. The outer wall is still there, but the lamellar bond that should connect it to the coffin bone has failed. What has filled the gap is a lamellar wedge: scar-like, pathological tissue that formed when laminitis tore wall and bone apart. The wall on top of it isn’t doing the structural job a healthy wall does, because it’s anchored to disease, not to bone. Preserving the whole assembly doesn’t preserve your horse’s foot. It keeps the lever long and the lamellar bond under continued stress, stride after stride.
Here’s the bit worth holding on to. If you’ve watched conventional farriery fail your horse, your frustration is legitimate. The protocol gets traction precisely because conventional care without proper radiographs is genuinely unsatisfactory. The answer isn’t no professional care. It’s better-coordinated professional care: a vet and a farrier working together from current marked radiographs, with measurements you can read and a plan you can ask questions about. The rest of this article shows you what that looks like, and what to ask for if your horse isn’t getting it.
Why the lever bit matters more than it sounds
Think about opening a heavy door. Push on the handle, far from the hinge, and the door swings easily. Push right next to the hinge and it barely moves. Same force, very different result, because of where you’re pushing.
That’s what happens at the coffin joint inside your horse’s foot at every stride. As the heel lifts and the foot rolls forward over the toe, the ground is “pushing” against the front of the hoof. The further forward that push is (in other words, the longer the toe), the bigger the twisting force on the coffin joint inside, and the harder the deep flexor tendon has to pull to keep things stable. That tendon runs straight across the back of the navicular bone. So every time the horse breaks over a too-long toe, the navicular bone takes the hit too.
This isn’t speculation. It’s been measured, in real horses, by multiple research groups over the last twenty-five years.¹,²,⁷ It’s why squared toes, rolled toes, and rocker toes work in horses with palmar foot pain. It’s why every evidence-based therapy for navicular syndrome involves shortening that lever. A protocol that denies the lever exists is denying the mechanism on which the entire therapeutic literature for foot pain is built.
The 0.2 mm answers the wrong question
The 0.2 mm figure is real. The post calculates it correctly: that’s roughly how much the bottom edge of the toe wall deflects at the canter. Small. Less than the thickness of a fingernail. Almost certainly not, by itself, doing any harm.
But it’s the wrong measurement for the question that actually matters. The mechanism of damage in laminitis isn’t the wall bending at its distal edge. It’s the tensile force pulling on the lamellar bond that holds the wall to the coffin bone. That force isn’t measured in millimetres of wall deflection. It’s measured in kilonewtons of deep flexor tendon tension, driven by the long lever arm we keep coming back to.
When researchers actually look at what loads the lamellar bond, they don’t measure how far the wall flexes. They measure the moment arm at the coffin joint, the tendon tension that results, and the load transferred onto the lamellar interface through every stride. A 10 mm change in toe length shifts those forces by around 20 per cent. That is the number that matters for your horse. The 0.2 mm isn’t wrong. It’s just answering a question nobody serious was asking.
The wedge isn’t the wall
Here is the single most important thing in this article. If you take nothing else from it, take this.
When you look at a chronic laminitic foot from the side, you see a long, often slipper-shaped toe that has grown out at the wrong angle. The new hoof wall is coming down from the coronary band at a healthier angle, and below it is the older, distorted toe.
The protocol being defended online tells you that this older, distorted toe is “the toe wall”: a structural part of the foot, a “pillar of support” that should be preserved at all costs.
It isn’t.
What’s actually sitting between the outer wall you can see and the coffin bone inside your horse’s foot is something called a lamellar wedge. It’s the pathological tissue that forms when laminitis tears apart the bond between the hoof wall and the bone. It is made of stretched, disrupted, scarred connective tissue and disorganised horn. It is not structural. It cannot transfer load between the wall and the bone the way a healthy lamellar bond does. It is, in plain terms, the disease, not the structure.
Think of it this way. Imagine a fingernail that has partly lifted away from the finger, and the gap between them has filled with a layer of dead, fibrous scar tissue over time. Would you call that scar tissue “the fingernail”? Would you protect it as a structural part of the hand?
That’s what’s being preserved when the protocol tells you not to take the toe back. The outer wall is still there, but it’s no longer doing the structural job the protocol claims. Beneath it sits a fibrous wedge of pathological tissue that grew when the lamellar bond between wall and bone failed. Wall without that bond is wall without a job. The protocol is preserving the assembly and calling it a pillar of support.
And here’s where the two things connect. By preserving that wedge, you’re keeping the effective toe long. And by keeping the toe long, you’re keeping the lever long. Every stride, more force on the deep flexor tendon. More force on the navicular bone. More tension on the lamellar bond that’s trying to grow back together at the top.
The protocol denies that the toe is a lever because that’s the only way the wedge can be preserved without admitting that preserving it perpetuates the original damage.
“But the horse needs three points of support”
You’ve probably read the version of this argument that says the horse needs to stand on “the two heels and the toe,” and that taking the toe back will “dump weight onto the sole under the coffin bone.”
The horse’s foot doesn’t work like a tripod. The weight-bearing surface is the entire ground perimeter of the foot: the heels, the bars, the frog, and the wall around the outside. Pressure measurements taken in actual horses on actual force plates show that the heel region typically bears the largest single fraction of the load, around 30 to 45 per cent, with the rest distributed around the foot.³ At no point in a stride does the foot bear on three discrete points.
And the bit about “dumping weight onto the sole under P3” sounds frightening but misses what radiographically guided farriery actually does. A good farrier and vet working from current radiographs aren’t choosing between “long toe” and “thin sole at the tip of P3.” They’re measuring sole depth, palmar angle, rotation, and other things, and choosing a trim and a shoe that protects the sole: wide-web shoes, wooden shoes, glue-on shoes, frog support, whatever the horse in front of them needs.⁴ The protocol turns a sophisticated, measured decision into a false binary, and uses that false binary to justify doing very little.
You weren’t wrong to lose faith. But the fix isn’t this.
Here is something that needs saying directly, because the online community in question is built on it.
If you’ve watched your horse get progressively worse under conventional farriery, your frustration is real. Conventional farriery on a laminitic horse without radiographs is genuinely unsatisfactory. Long-toe low-heel farriery in particular (leaving toes too long for too long) is one of the most reliably documented contributors to lamellar stress in horses that go on to develop or relapse with laminitis.¹,² That isn’t a guess. It’s been measured and replicated for decades.
But here’s the inversion the protocol relies on. It tells you that shortening the toe was what caused the distortion. It wasn’t. The mechanism of harm in chronic LTLH conformation is the opposite: the toe was allowed to grow too long, for too long, and the deep flexor tendon and the lamellar bond paid the price stride after stride after stride.
The slipper-toed foot you see in a chronic laminitic horse is the historical record of months or years of that loading pattern in a foot whose lamellar bond was already failing. The wedge being grown out is the evidence. The new wall coming down at a healthier angle from the coronary band is what good corrective trimming makes possible. It is not something the protocol invented.
The answer to bad farriery isn’t no farriery. It’s better-coordinated farriery, guided by current radiographs, with a farrier and a vet who talk to each other.
What “the X-rays show it’s working” needs to actually mean
The yards promoting this protocol take radiographs. They post them. They tell owners the lamellar attachment is regenerating, the rotation is correcting, the horse is improving. To an owner who has been told their previous vet was wrong, this looks like proof.
Three things matter here, and you can use them as a checklist.
First, a radiograph only means something if it’s measured. The relevant measurements in laminitis are the lamellar lucent zone (the gap between the inner hoof wall and the coffin bone, which directly reflects lamellar separation), the founder distance, the rotation angle, the palmar angle, and the sole depth. Marked weight-bearing radiographs taken to a standard protocol allow these to be measured properly.⁵,⁶ A photo of a foot with a radiograph in the background is not a measurement.
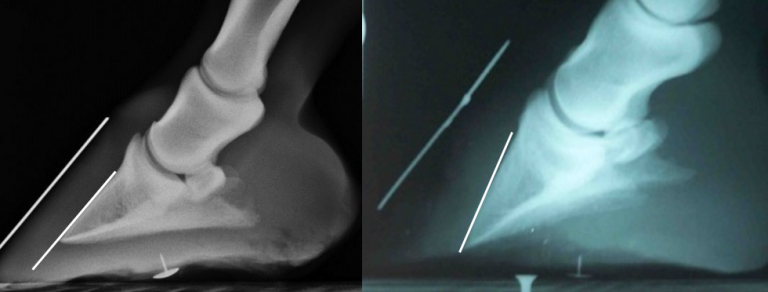
normal on left, rotated P3 on right. Note difference in divergence
Second, the most direct measure of whether the lamellar attachment is regenerating is the lamellar lucent zone. It measures from the inner hoof wall, so it isn’t affected by what the trimmer did to the outer wall. If the LLZ is reducing on successive radiographs, that’s real evidence. If the only evidence is that the outer hoof wall looks better, that’s the protocol grading
its own homework: the outer wall looks the way it does because that’s what the protocol was designed to produce.
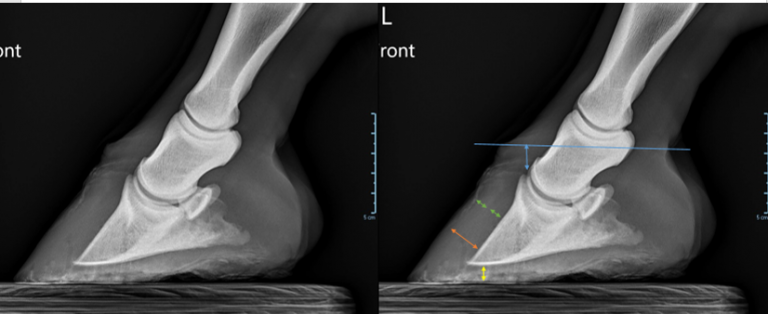
Sinking is indicated by the increased distance between P3 and coronary band (blue), hoof capsule is < 1/2 of total hoof wall (green), total distance from P3 to dorsal wall is greater (orange), sole distance is smaller (yellow)
evidence of sinking – shelf at coronary band due to downward movement of P3; distance from P3 process to coronary band is increased
rotation, phalangeal alignment is best described as hoof capsule divergence whilst flexural deformation at the DIPJ such as that in the right image is true rotation
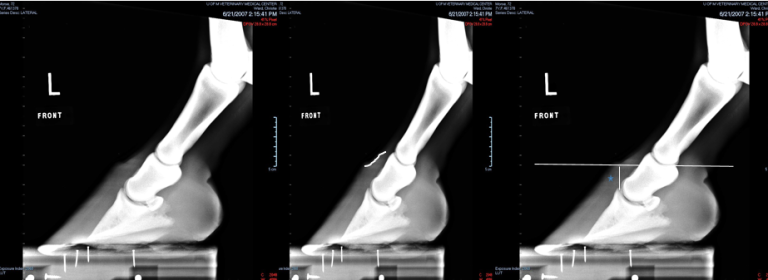
evidence of sinking – shelf at coronary band due to downward movement of P3; distance from P3 process to coronary band is increased
Third, radiographs in laminitis need to be interpreted by a vet. Not by the trimmer who took them. Not by the owner. Bone changes, the risk of solar penetration, the early warning signs of supporting limb laminitis in the other foot: these aren’t things the average owner or trimmer can spot. They are why veterinary involvement in laminitis is not optional.
So if your horse is being rehabbed and you’re being shown radiographs as proof, the question to ask is: who measured them, what did they measure, and how do the measurements compare to the last set? If the answer is some version of “the foot looks better,” that isn’t an answer.
The horses we’re worried about
If you spend time in the comment threads where this argument circulates, you meet the horses being managed under it. Some are doing fine. Some are not. A few stand out.

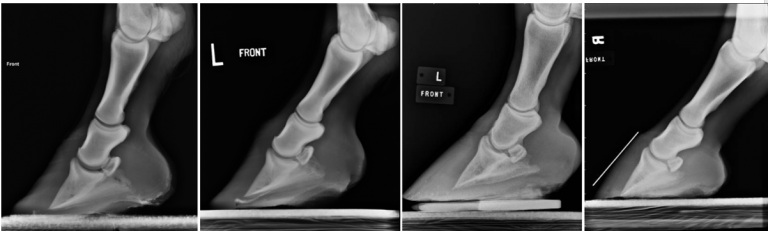
not all cases respond to any given treatment protocol in the same way and appropriate veterinary monitoring are strongly advised.
A pony on a remote Scottish island with a toe that’s curling upward away from the ground. The owner is trimming him herself. There is no vet who can get to her, no farrier on the island, and the ferry runs only when the weather allows. She’s been told by the yard that the upward curl indicates “loss of P3.” That is, in fact, a serious clinical finding that needs veterinary investigation. She is being supported in continuing self-trimming as the management response.
An owner posting that she is rehabbing not just her own horse but multiple friends’ horses under this method, with no veterinary or qualified farrier involvement, and that the protocol is “absolute best way to rehab laminitis.”
An owner saying she had a previous horse die of laminitis “doing everything the vet and farrier said,” and that this method works for her now. The grief is real. The conclusion she has reached, that the vet and farrier were the problem, is the conclusion that protocol-led communities are designed to produce.
None of these owners are the cause of the problem. They are doing their best for horses in their care. Several of them are doing it in isolation, geographically or socially, and the online community has stepped into a gap that conventional care left open. That’s worth saying plainly. It’s also worth saying plainly that the horses themselves are at risk, because the protocol they’re being managed under does not include the surveillance that the evidence base for laminitis rehabilitation requires.
What to do if any of this rings true for your horse
If your horse is being rehabbed under this method, or you’ve been told by someone you trust online that toe length doesn’t matter, here is a short list of questions to ask.
● When were the last marked weight-bearing radiographs taken of both forefeet? (“Marked” means with a metal pin or tape on the dorsal hoof wall and at the coronary band, so the inside of the foot can be related to the outside.)
● Who is measuring them? A veterinary surgeon, ideally one with equine podiatry experience, should be the one reading and measuring the films.
● What are the actual numbers? Lamellar lucent zone, founder distance, rotation angle, palmar angle, sole depth. Ask for them in writing. Ask for the comparison to the previous set.
● Is the sole depth above 12 mm? This matters because below that, the tip of the coffin bone is at risk of pushing through. It governs how aggressively the foot can be trimmed at any given session.
● Is the trimming being done by a registered farrier, or under the direct guidance of one, in consultation with the vet?
● If your horse is overweight, on grass, or has a history of insulin dysregulation, has an endocrine assessment been done? Laminitis driven by metabolic disease will not stay fixed unless the metabolic disease is treated, regardless of how the foot is trimmed.
If the answer to most of these is “no” or “I don’t know,” the management your horse is on is not aligned with the published evidence base, no matter what’s being said in the Facebook group.
That isn’t an attack on you. It’s an invitation to ask for more.
A final word
The toe is a lever. The wedge is not the wall. The foot doesn’t load on three points. The cause of post-laminitic distortion is long-toe loading, not the correction of it. And radiographic guidance, by a vet who measures and a farrier who acts on those measurements, is what separates a horse on a real recovery path from a horse being managed by hope.
If you’ve lost faith in conventional care after a bad experience, that experience was real and the answer isn’t to pretend it wasn’t. The answer is to demand the version of conventional care that the evidence base actually points to: a farrier and a vet, working together, with current marked radiographs and a documented plan that you can read and ask questions about. That’s not a higher standard than your horse deserves. It’s the floor.
Share this with anyone you know who might be heading down the other road. The horses involved can’t make this argument themselves.
Where the numbers in this article come from
For owners who want to read further, or vets and farriers who want to check the references:
1. van Heel MCV, van Weeren PR, Back W. Shoeing sound Warmblood horses with a rolled toe optimises hoof-unrollment and lowers peak loading during breakover. Equine Veterinary Journal 2006;38(3):258–262.
2. Eliashar E, McGuigan MP, Wilson AM. Relationship of foot conformation and force applied to the navicular bone of sound horses at the trot. Equine Veterinary Journal 2004;36(5):431–435.
3. Rogers CW, Back W. The effect of plain, eggbar and 6 degrees-wedge shoes on the distribution of pressure under the hoof of horses at the walk. New Zealand Veterinary Journal 2003;51(1):19–23.
4. Parks AH, O’Grady SE. Chronic laminitis: current treatment strategies. Veterinary Clinics of North America: Equine Practice 2003;19(2):393–416.
5. Skelton K, Acutt E, Stefanovski D, van Eps AW. The lamellar lucent zone: a novel radiographic measurement for the diagnosis of acute laminitis in horses. Equine Veterinary Journal 2024.
6. O’Grady SE, Parks AH. Farriery options for acute and chronic laminitis. AAEP Proceedings 2008;54:355–363.
7. Willemen MA, Savelberg HHCM, Barneveld A. The effect of orthopaedic shoeing on the force exerted by the deep digital flexor tendon on the navicular bone in horses. Equine Veterinary Journal 1999;31(1):25–30.
8. Wilson AM, McGuigan MP, Su A, van den Bogert AJ. Horses damp the spring in their step. Nature 2001;414:895–899.