
What the “Drop the Heels” Protocols Aren’t Telling You About Your Laminitic Horse
Produced by the HoofFlix Team; Dr. Mark Caldwell PhD; FWCF., Neil Madden FWCF., Sam Fowler DiP WCF’
A clinical argument for owners and semi-professional trimmers who want to understand what heel height actually does inside the foot — and why getting it wrong, in either direction, has consequences that outlast the trim.
There are two ways to get heel height wrong in a laminitic horse. The first is the way conventional farriery has been getting it wrong for decades: leaving the heels too low for too long, allowing the toe to creep forward, and failing to maintain the palmar angle of the coffin bone within a safe range. That is a real problem. The research literature is clear about it, and many horses have paid for it.
The second way is less discussed, but the horses paying for it are just as real. It is the protocol that drops the heels aggressively, often to near-ground level, and holds them there as a matter of philosophy rather than measurement. The argument given is that this restores a “natural” hoof geometry. The anatomy, the biomechanics, and the radiographs say something more complicated.
This article works through both ends of the problem. It explains what heel height actually does to the structures inside your horse’s foot, why there is a therapeutic range with hard limits in both directions, and what the evidence says about the pace and degree of heel change that is safe in a foot whose lamellar attachment is already compromised. It is aimed at owners managing laminitic horses and at semi-professional trimmers who have learned a method but want to understand the physics behind it.
The same framework that explains why heels should never be left low also explains why dropping them fast and far is dangerous. The two arguments are made of the same mechanics. That is not a coincidence.
The Anatomy You Need First
Inside your horse’s foot, three structures are doing most of the load-bearing work, and heel height affects all three directly. You need to know what they are before any argument about trimming makes sense. The coffin bone — P3, the distal phalanx — is the structural core. The entire hoof capsule is built around it. Its upper surface is bonded to the inner face of the hoof wall through the lamellar junction, Velcro-like interface of interlocking microscopic leaves of sensitive and insensitive lamellae. This junction carries the horse’s full body weight in suspension: it resists the tendency of P3 to push down and forward through the sole every time the horse bears weight. In laminitis, that junction is what fails. When it fails at the toe, P3 rotates. When it fails uniformly around the whole circumference, P3 sinks. The two can happen together, and in the worst cases, they do.
The deep digital flexor tendon — the DDFT — runs down the back of the leg, wraps around the navicular bone at the back of the foot, and attaches to the underside of P3. Its job is to flex the coffin
joint: to resist the tendency of the ground reaction force to push P3 backward and downward with every stride. The harder it has to work — the greater the force trying to extend the coffin joint — the more tension it carries. That tension has a direct physical relationship with heel height, and that relationship is
central to everything in this article.
The navicular bone sits behind P3, nestled between the back of the coffin bone and the DDFT. It functions as a pulley: the tendon wraps around its lower surface, changing direction to reach its
attachment on P3. As a pulley, it absorbs a compressive force — the resultant of the tension on both sides of the bend. The steeper the angle at which the DDFT approaches the navicular bone, the sharper the bend, and the greater that compressive force. Heel height directly controls that approach angle. Lower heel: steeper angle, more compression. Higher heel: shallower angle, less compression.
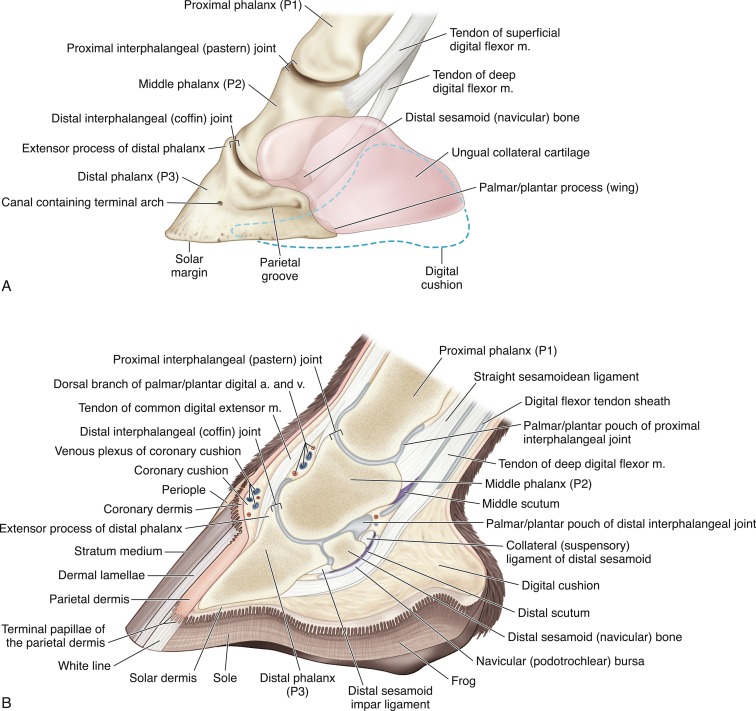
Fig 1. Detailed anatomy of the equine foot
The palmar angle of P3 ties these three together. It is the angle between the bottom surface of the coffin bone and the ground, measured on a weight-bearing lateromedial radiograph. The normal range in a forelimb is 3 to 5 degrees positive: the heel end of the bone sits slightly higher than the toe end. This geometry positions the DDFT at its designed working tension and keeps the sole of P3 at a safe distance from the ground. When the palmar angle falls below 2 degrees, the sole over the coffin bone tip starts to thin and bruising becomes likely. When it goes negative — when the toe end of P3 is higher than the heel end — that is, in the plain language of the research literature, a clinical emergency.
In a laminitic horse, the palmar angle is the single most important number a farrier can know. Everything that follows from here is about how heel management affects it, and what happens when that management goes wrong.
What Heel Height Does to the DDFT
Here is the mechanism that connects heel height to tendon loading, stated plainly.
The ground reaction force acts upward through the horse’s foot at a point called the centre of pressure — roughly 9.5 mm behind the frog apex at mid-stance. The coffin joint has its pivot point — the centre of rotation — further back, closer to the middle of the foot. The distance between where the ground pushes and where the joint pivots is the moment arm: the mechanical advantage the ground has over the joint. The DDFT has to generate enough tension to counterbalance that moment every step. The bigger the moment arm, the harder the tendon works.
Heel height modifies this geometry. As the heel drops, the palmar angle of P3 decreases, the bony column tilts, and the moment arm lengthens. The centre of pressure shifts forward relative to the joint. The DDFT has to work harder. The evidence puts a number on it: in a 500 kg horse, each degree the heel drops below the reference angle increases DDFT tension by approximately 75 to 100 Newtons.¹ Drop the heel 5 degrees below the reference angle and the DDFT is carrying 375 to 500 N above its designed working load — every step, every day. In a horse doing 10,000 strides a day, that is not a small number. It is an accumulated injury.
This is the mechanism behind long-toe low-heel syndrome. It is why horses managed in that conformation develop progressive deep digital flexor tendinopathy. It is why the research consistently
shows that the conventional farriery failure mode — leaving the heels too low for too long — damages the tendon and the navicular bone over time. Nobody who has read the force plate literature disputes this.
But the same formula works in both directions.
What Happens When You Drop the Heels Fast, or Too Far
The protocols in question do not generally advocate for keeping heels permanently low. What they do is advocate for dropping them quickly, often in a single session or over a short period, to reach a target geometry that may not have been arrived at with any measurement of the actual palmar angle of P3 in that individual horse.
Here is what the biomechanics says about that approach. When you lower the heel, you do two things simultaneously. You decrease the palmar angle of P3, and you increase the length of the moment arm through which the DDFT is working. Both of those changes increase DDFT tension. In a normal horse whose lamellar junction is intact, the DDFT under increased tension is being pulled against an anchor that is structurally sound. The bone does not move. The tendon stretches in its elastic range and returns.
In a laminitic horse whose lamellar junction has partially or fully failed at the dorsal toe, the DDFT under increased tension is being pulled against a compromised anchor. The force that the tendon exerts on P3 is the same force that is trying to rotate the coffin bone further away from the dorsal wall. Every increment of additional DDFT tension applied by dropping the heels is, in a rotated laminitic foot, working in exactly the direction the disease has already started pulling. It is not correcting the rotation. It is loading the mechanism that drives it.
“The DDFT is under increased tension in the laminitic foot, and rapid heel lowering in a single session loads the already-compromised lamellar attachment.”² The three-degrees-per-session rule for palmar angle correction — the maximum safe change at any single trimming visit — exists precisely because of this mechanism. It is not a conservative preference. It is a biomechanical limit derived from the same force calculations that define what the lamellar junction can withstand.
A foot arriving at the farriery with a negative palmar angle of 5 degrees requires two to three sessions to correct safely, not one. Each session reduces the deficit by 3 degrees maximum. Not because it would be inconvenient to do it faster, but because doing it faster loads a structure that is already failing.
A protocol that drops the heels aggressively in a single session — or that demands ground-level heel height as the target geometry regardless of the individual horse’s radiographic measurements — is not working within this limit. It is overriding it.
The Navicular Bone Is Not a Bystander
The navicular bone’s role in this process is worth spelling out separately, because it is where some of the most permanent damage in the laminitic horse can accumulate silently.
As the DDFT tension increases with falling heel height, the compressive force on the navicular bones’ flexor surface increases in proportion. The DDFT approaches the navicular bone at a steeper angle as the heel drops, sharpening the bend it makes around the bone’s surface and increasing the resultant compressive force pushing into it.³ The fibrocartilage on the navicular bones’ flexor surface — the material being compressed — adapts slowly to increased load and tolerates sustained overload poorly. It does not inflame the way a tendon does. It erodes. And because erosion accumulates over time before it becomes visible on radiograph, the first sign you may see is a finding on MRI that represents months of cumulative damage.
This is why heel height matters in navicular disease, and why the same DDFT mechanics that govern laminitis management also govern navicular management. They are the same tendon, the same pulley, the same compressive geometry. A protocol applied to a laminitic horse that aggressively lowers the heels is not applying laminitis management. It is, from the navicular bones’ perspective, applying the same loading pattern that causes navicular syndrome. In a horse recovering from lamellar failure, this is not a background concern. It is a foreground one.

Panel 1 — Low / collapsed heel shows the DDFT taking a steep approach angle around the navicular bone (maximising compressive force on its flexor surface), the GRF acting far forward of the joint centre (long moment arm ~22 mm), and P3 sitting at a near-zero palmar angle. The force numbers — +375 to +500 N above baseline for a 5° heel deficit — come directly from the Biomechanics for Farriers 75–100 N per degree rule.
Panel 2 — Reference heel shows the DDFT at its designed working angle, the moment arm shortened to ~15 mm, and P3 sitting at its reference 3–5° palmar angle. This is the geometry the lamellar attachment is built to tolerate.
Panel 3 — Therapeutic elevation shows what a correctly applied wedge achieves: the approach angle flattens further, navicular compression falls, and DDFT tension drops by approximately 20–24% (6° correction × ~4% per degree). The wedge is shown explicitly beneath the heel. The warning about chronic elevation and heel contraction risk is included because the Equine Foot Vol 2 is clear that elevation is a staged, titrated intervention — not a permanent state.
The 3°/6 mm per session safe correction limit appears in the Panel 3 data box, with the same rationale the article uses: the DDFT is already under altered tension in the laminitic foot, and the lamellar attachment cannot accommodate rapid mechanical change within a single trimming cycle.
Two Problems at the Same Time: Pain and Divergence
The discussion above covers the structural damage that aggressive heel lowering can cause over time. But there is a more immediate consequence that matters in the horse you are standing in front of today.
Dropping the heels acutely, beyond the 3-degree safe limit per session, increases DDFT tension acutely. In a horse whose coffin joint and navicular bone are already sensitised by active or recent inflammation, that acute increase in DDFT tension and navicular compression is experienced as pain. This is measurable and reproducible. It is why horses with navicular pain point their forefeet — heel raised off the ground, toe bearing weight — to offload the DDFT. The raised heel reduces tendon tension; the horse is instinctively seeking the geometry that hurts less.
When a trimmer drops a laminitic horse’s heels beyond what the individual palmar angle and DDFT tension state can accommodate, the horse does not improve in the hours and days following the trim. It gets worse. The owner reports that the horse seemed more uncomfortable after the trim. The explanation offered by the protocol is usually that this is expected soreness, part of the process, evidence of realignment. Sometimes it is. Sometimes it is a sign that the trim has loaded a compromised structure beyond its tolerance threshold.
The difference matters enormously, and the only way to tell them apart reliably is radiographic measurement of the palmar angle before and after. Without that measurement, “expected soreness” and “we just damaged this horse” look identical from the outside.
The second consequence is divergence. In rotational laminitis, the DDFT tension is the mechanical force trying to pull P3’s toe further away from the dorsal hoof wall. It is the vector driving the rotation. Anything that increases that tension — including dropping the heels beyond the safe correction limit — adds force to the rotational vector. Over multiple sessions of excessive heel lowering, the palmar angle decreases further, the DDFT tension increases further, and the rotation progresses. The lamellar wedge, the pathological tissue that fills the space between the separated wall and P3, becomes larger. The founder distance — the gap from the coronary band marker to the extensor process of P3 — increases.
This is how a horse managed under an aggressive heel reduction protocol can show progressive radiographic worsening while the trimmer and the owner believe they are improving the situation. The outer geometry may look different. The toe line may have changed. The hoof pastern axis may appear straighter from the outside. But on a marked weight-bearing lateromedial radiograph with measurements, P3 may be further from the dorsal wall, lower in the capsule, and closer to the sole than it was before the protocol began.
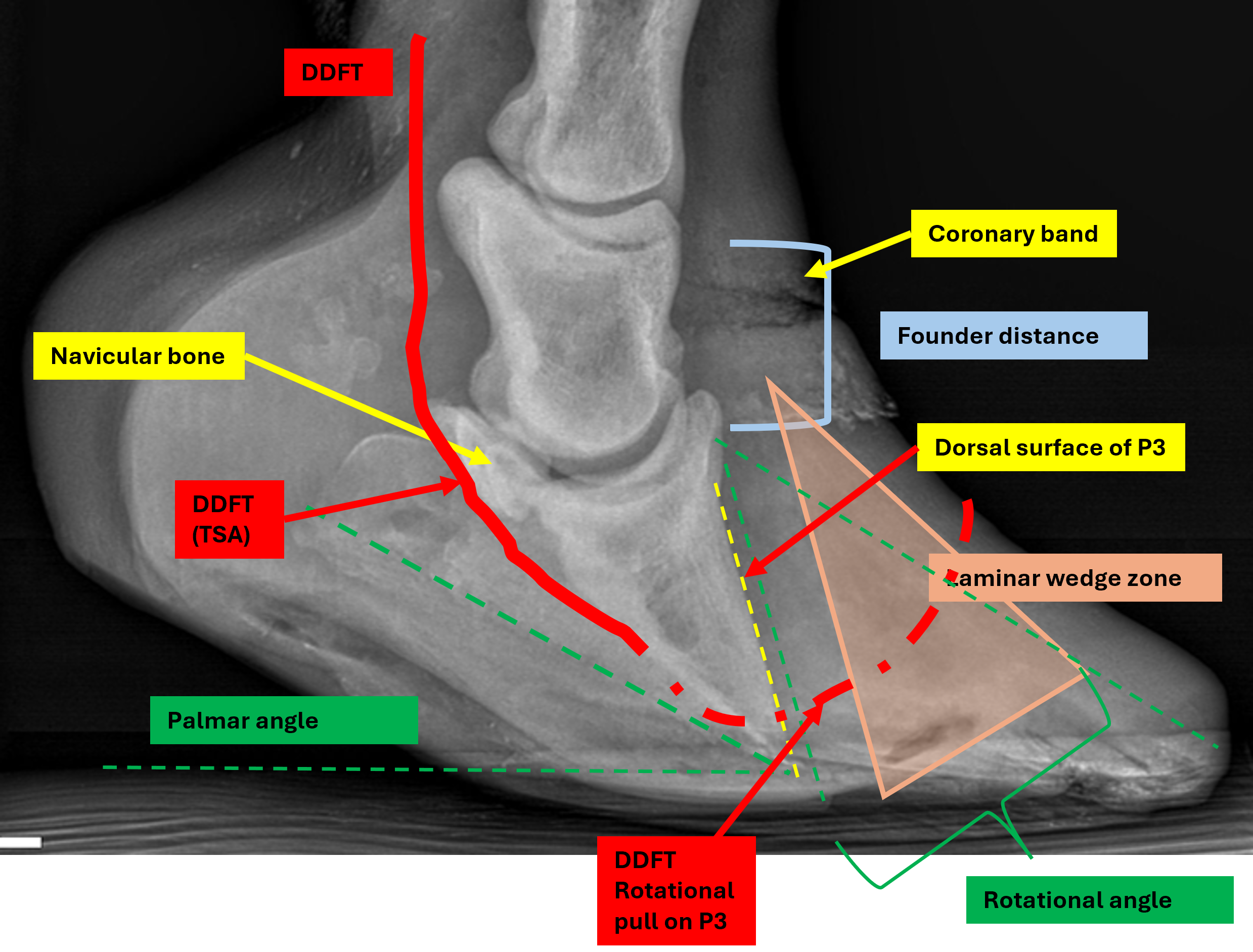
Yellow dashed line — the dorsal surface of P3 (coffin bone). The visible angular divergence between these two lines is the rotation angle — the direct radiographic evidence of lamellar failure at the toe.
Green bracket — the rotation angle measured mid-toe, showing the gap between outer wall and P3 that has opened as rotation has progressed.
Orange shaded zone — the lamellar wedge, the pathological fibrous tissue occupying the space between the separated wall and the bone surface. The wider this zone, the greater the lamellar failure.
Cyan bracket — the founder distance, measured from the coronary band marker level down to the extensor process of P3. As rotation and sinking progress under continued DDFT loading, this distance increases.
Red line — the DDFT path running down the back of the digit, curving around the navicular bone and attaching to the solar surface of P3.
Bold red arrows at the toe — the DDFT rotational pull vector, showing the mechanical direction in which increased DDFT tension acts — pulling the toe of P3 further away from the dorsal wall and driving progressive divergence.
Green dashed line — the solar border of P3, illustrating the palmar angle relative to the ground reference line (white dashes).
You cannot see that without radiographs. And you cannot safely manage a laminitic horse without them.
The Case for Heel Elevation, and Its Limits
The argument so far might seem to be pushing toward the opposite extreme: raise the heels high and leave them there. It is not. The therapeutic role of heel elevation in laminitis management is real, measured, and specific — and it, too, has limits in both directions.
In a horse with a negative or very low palmar angle following lamellar failure, the DDFT is under pathologically elevated tension. The toe of P3 is being pulled toward the ground. Heel elevation directly counters this: raising the heel increases the palmar angle, shortens the effective moment arm, and reduces DDFT tension in a calculable and proportional way. The research evidence for this is the same evidence that condemns long-term low heels: each degree of heel elevation provides a measurable reduction in DDFT tension.¹ It is the same formula applied in the therapeutic direction.
But excessive heel elevation has its own consequences. Raising the heels loads the DDFT in a shortened functional position. Over time, chronic elevation without monitoring and progressive reduction can contribute to contraction of the heel and loss of frog ground contact. The digital cushion, which depends on frog loading to maintain its fibrocartilaginous density, is denied the cyclic compression that sustains it. In the longer term, this makes the heel structures less capable of absorbing load, not more. Heel elevation in laminitis management is a staged intervention, not a permanent state. It is titrated against the palmar angle on successive radiographs and progressively reduced as the palmar angle restores and new, well-attached hoof wall grows down from the coronet.
The safe range is not a matter of opinion. It is a consequence of the same biomechanics. The target palmar angle for a forelimb is 3 to 5 degrees positive. A palmar angle below 2 degrees is dangerous. A negative palmar angle is a clinical emergency. The heel height required to maintain the palmar angle within the safe range varies with every individual horse’s conformation, the degree of P3 displacement, the sole depth, and the shoeing interval. There is no single number that is right for every horse. There is only the measurement.

heel elevation post trim in the form of an additional variation to a therapeutic device, such as the clog , relieves DDFT tension and laminal shearing during the stance phase. The degree of elevation is calculable by the measurement data from radiographs.
What “Rapid Correction” Really Means
The phrase “rapid heel lowering” appears in the evidence-based literature as a risk category, not a technique. It refers to any change in heel height that moves the palmar angle beyond 3 degrees per session — whether that is lowering too fast or, in the rare case of a horse that has been inappropriately wedged, raising too fast. The limit exists because the tissues being loaded cannot adapt within a single shoeing cycle to the change in their mechanical environment.
For a laminitic horse managed under a protocol that sets heel height by philosophy rather than by palmar angle measurement, rapid correction is essentially the default. Without a measured baseline, without a target angle, without radiographic confirmation of where P3 is sitting, there is no framework for knowing how much heel change is too much. The trimmer is working from appearance and from a set of rules that do not include the variable that governs the safe rate of change.
This is not a criticism of the intent. Many of these trimmers care deeply about the horses they are working on. The problem is structural. A trimming protocol that does not include radiographic
measurement of the palmar angle before and after any significant heel change is not a laminitis management protocol. It is a hoof management protocol being applied to a laminitis case. The two are not the same thing, and the horse in front of you cannot tell you which one you are doing.
Vertical Displacement: The Sinker
Rotational displacement of P3 is the failure pattern most people think of with laminitis. But in a large proportion of presentations — particularly in severe or rapid-onset cases, and in horses managed under protocols that apply significant load to an already-failing lamellar junction — P3 can sink distally without rotating, or sink in combination with rotation. The horse’s digital venography shows filling defects around the whole circumference, not just at the toe. The founder distance increases uniformly. The coronary band drops toward the ground on both sides simultaneously.
Sinking is caused by uniform lamellar failure around the perimeter. Any management approach that increases load on the lamellar junction without distinguishing between which regions of that junction are still competent and which have failed risks converting a rotational presentation into a combined rotational and sinking one. Venography, which maps which parts of the lamellar circulation are still perfused, is the only tool that identifies this distinction before the clinical picture makes it obvious.
The relevance to aggressive heel reduction is direct. In a foot where the lamellar junction is failing not just at the dorsal toe but more broadly, loading the DDFT to increase palmar tension by dropping the heels adds compressive stress through P3 onto a lamellar surface that may have less reserve than the outward appearance of the foot suggests. There is no way to assess that reserve from the outside. The venogram tells you. The radiograph tells you the bone position. Neither of these is optional in a laminitic horse, and neither is provided by a trimming-only protocol.

True sinker and total vertical displacement of P3 within the hoof capsule
The Trimmer, the Vet, and the Measurement That Connects Them
The protocol being described in this article — aggressive heel reduction, high frequency trimming, no radiographic measurement, no veterinary co-management — is built on a coherent internal logic. The argument is that the foot knows what it is doing, that the correct geometry will reveal itself if you remove the interference of shoes and excessive structure, and that veterinary and farriery involvement has been the cause of more damage than it has prevented.
On the last point, it is worth being honest: that argument has purchase in specific cases because it is sometimes true. Conventional management without radiographic guidance, long shoeing intervals, and failure to maintain the palmar angle within the reference range have damaged a large number of laminitic horses over decades. The anger at those failures is legitimate.
But the answer to management without measurement is not management with different rules and still no measurement. It is management with better measurement. The palmar angle of P3 is not a veterinary abstraction. It is the number that tells you whether what you just did made things better or worse. Without it, every intervention — however carefully rationalised, however confidently described — is untethered from the structure it is supposed to be helping.
The three-degrees-per-session rule exists because of the physics. The maximum safe correction rate applies whether you are raising the heels or lowering them. The radiographic check before and after any significant trim change is not a formality. It is the mechanism by which a trimmer knows whether they are moving toward the reference range or away from it.
If the horse you are managing is getting trims at the frequency described by these protocols, the trimmer is touching those heels regularly. That is a lot of opportunities to measure. Radiographs at the start of rehabilitation, before any significant heel change, and after each shoeing cycle until the palmar angle is stable within the reference range, is not an unreasonable standard of care for a condition in which P3 is or has been displaced. It is the standard of care the published evidence points to.
A Final Word
Getting heel height right in a laminitic horse is not simple. It requires knowing where P3 is, what direction it has displaced, what the current palmar angle is, how much sole depth remains above the coffin bone tip, and what the DDFT tension state of the individual horse is in this foot at this moment. None of those things are visible from the outside. All of them are obtainable from a correctly taken marked lateromedial radiograph interpreted by a veterinary surgeon and communicated to the farrier.
The claim that heels should be dropped aggressively in laminitic horses because it is more natural is a claim about geometry. The claim that heels should be dropped without radiographic measurement is a claim about what you need to know to do it safely. Both claims are wrong, and the cost is borne by the horse.
The mechanics do not care about the philosophy behind the trim. The DDFT does not respond to the theoretical framework of the method. The lamellar junction fails under load, and it does not distinguish between load applied from a bad intention and load applied from a good one. It responds to force. And force, in the equine foot, is subject to physics that can be calculated, measured, and managed — but only if you have the measurements to manage it with.
The answer to bad management is not different management. It is measured management. The tools exist. The evidence is there. The horse in front of you is waiting for someone to use them.
Where the Numbers in This Article Come From
For owners who want to read further, or trimmers who want to check the references:
1. Caldwell M, Madden N. *Biomechanics for Farriers*. Scientific Horseshoeing Limited. [Unpublished pre-publication draft, 2025]. Chapter 2: The loaded foot — DDFT tension, heel angle, and the 75–100 N per degree rule in a 500 kg horse; Formula F1 for heel elevation calculation; three-degrees-per-session correction limit.
2. Caldwell M, Madden N. *The Equine Foot: Science, Craft, and Clinical Reasoning in Farriery and Podiatry*, Volume 2. Scientific Horseshoeing Limited. [Unpublished pre-publication draft, 2025]. Chapter 28: Laminitis — phase-specific farriery, subacute trim protocol, safe rate of palmar angle correction, DDFT tension implications of heel lowering.
3. Eliashar E, McGuigan MP, Wilson AM. Relationship of foot conformation and force applied to the navicular bone of sound horses at the trot. *Equine Veterinary Journal* 2004;36(5):431–435.
4. van Heel MCV, van Weeren PR, Back W. Shoeing sound Warmblood horses with a rolled toe optimises hoof-unrollment and lowers peak loading during breakover. *Equine Veterinary Journal* 2006;38(3):258–262.
5. Willemen MA, Savelberg HHCM, Barneveld A. The effect of orthopaedic shoeing on the force exerted by the deep digital flexor tendon on the navicular bone in horses. *Equine Veterinary Journal* 1999;31(1):25–30.
6. O’Grady SE, Parks AH. Farriery options for acute and chronic laminitis. *AAEP Proceedings* 2008;54:355–363.
7. Skelton K, Acutt E, Stefanovski D, van Eps AW. The lamellar lucent zone: a novel radiographic measurement for the diagnosis of acute laminitis in horses. *Equine Veterinary Journal* 2024. [Epub ahead of print, doi:10.1111/evj.14436]
8. Morrison S. Outcome of deep digital flexor tenotomy in 245 horses with chronic laminitis. Cited in: O’Grady SE. *Chronic Laminitis: Current Farriery Management*. AAEP Proceedings 2011.