
“There is no connection between the DDFT and P3”
From the HoofFlix Team. Mark Caldwell PhD., FWCF;
This post forms a robust reply to a comment on our previous article on variations of trimming techniques around heel height in the treatment of laminitis.
Thank you for taking the time to engage with this in detail, and for sharing your clinical case — a recumbent 750 kg Friesian walking within 48 hours is a meaningful outcome and worth discussing seriously. That is exactly the kind of case the profession needs to reason about carefully rather than dismiss.
The overwhelming rate of evidence suggests the biomechanical argument you have made contains several errors that go to the heart of why this debate matters for horses being managed under protocols that do not include radiographic measurement. Let us work through them one by one.
“There is no connection between the DDFT and P3 because both are attached to the free end of the DDFM”
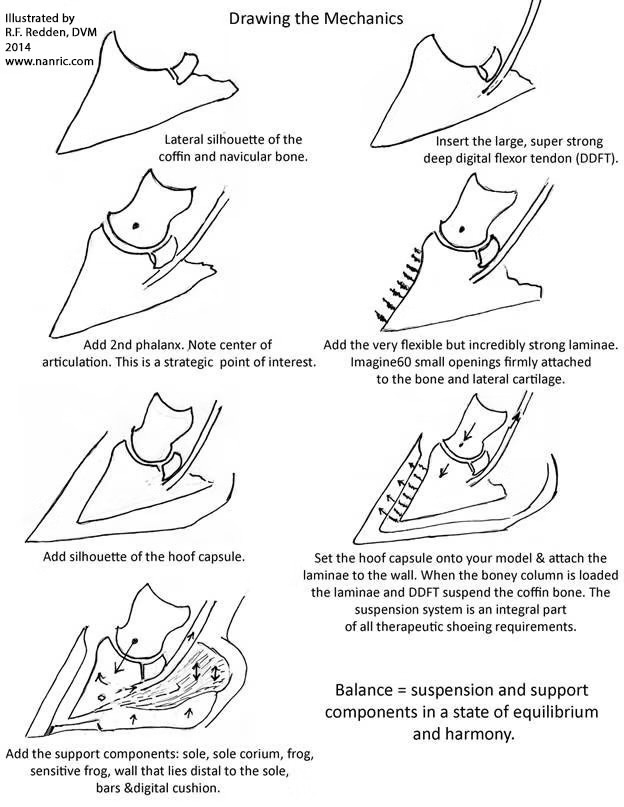
This is anatomically incorrect. The deep digital flexor tendon (DDFT) attaches to the semilunar crest on the solar surface of P3 — the distal phalanx. The deep digital flexor muscle (DDFM) is proximal; the tendon is its distal continuation. The tendon does not attach to the same point as the muscle belly. This is standard equine anatomy: the DDFM originates on the caudal radius and ulna, its tendon passes through the carpal canal, continues distally, wraps around the navicular bone, and inserts onto P3. These are two anatomically distinct points of attachment, and a tensile force transmitted through the tendon from the muscle to the bone is exactly what tendons are for.
The claim that both structures are “attached to the free end of the DDFM” describes a mechanical arrangement that does not exist in equine anatomy.
“The flexor muscle only fires when asked to — it is not pulling all of the time”
This is the most important error in the comment, and it is worth spending time on because it underpins the rest of the argument.
You are correct that the DDFM fires intermittently — it is a skeletal muscle under neural control. But the DDFT is not only loaded when the muscle fires. It is under continuous passive tension throughout stance, for three distinct reasons.
First: viscoelastic resting tone. Tendon and the musculotendinous unit retain passive stiffness at rest. The DDFT does not go slack when the muscle is not actively contracting. Like any connective tissue loaded in the anatomical position, it maintains a baseline tensile state. The magnitude of this passive tension is position-dependent — which is precisely why heel height matters.
Second: body weight transmission through stance geometry. During stance, the horse’s body weight acts downward through the column of bones — P1, P2, P3 — and the ground reaction force acts upward. If the DDFT were truly slack during stance, P3 would rotate freely under body weight with nothing to resist it except the dorsal lamellar attachment. That would mean a horse standing quietly would experience progressive coffin bone rotation from gravity alone, which demonstrably does not happen in horses with intact lamellar junctions. The DDFT provides continuous passive resistance to that rotational tendency throughout every moment of stance — not just when the muscle actively fires.
Third: the breakover phase. You are correct that the DDFT fires actively during propulsion — this is when DDFM contraction drives active flexion and the tendon tension peaks. This is also exactly the phase at which a long toe creates the maximum moment arm at the coffin joint, and at which the Van Heel and Eliashar force plate data were collected. A 10 mm shift in breakover reducing peak DDFT tension by 21 per cent refers to this active propulsive phase — which is when the highest forces occur.
The claim that the DDFT is only relevant when actively contracted treats it as a rope that is sometimes taut and sometimes coiled on the floor. That is not how tendons work. A tendon under passive tension in a loaded limb is transmitting force regardless of whether the muscle is firing. The distinction between active contraction and passive loading is meaningful in some contexts. In a weight-bearing stance analysis, it does not make the DDFT biomechanically irrelevant between footfall and toe-off.
“For the horse to rotate P3, the horse must pull the DDFM tight, then the Triceps, then the Serratus Cervicis”
This describes active, voluntary P3 rotation driven by the horse consciously engaging a muscle chain. That is not what the article describes, and it is not what happens in laminitis.
Rotational displacement of P3 in laminitis is not a voluntary muscular act. It is a structural failure. The lamellar junction — the biological velcro bonding the hoof wall to the periosteum of P3 — has a shear strength of approximately 2 MPa in healthy tissue. When the lamellar microcirculation is disrupted and enzymatic degradation of the basement membrane occurs, that shear strength falls. Body weight then acts through P3 via the bony column, and the DDFT’s continuous passive tension during stance acts on the solar surface of P3. When the degraded lamellar junction can no longer resist the combination of gravitational loading and tensile pull from the DDFT, P3 begins to displace.
This is not a horse choosing to fire its flexor chain. It is a structural element failing under a load it previously tolerated. The horse does not need to “want” to rotate its coffin bone any more than a bridge beam needs to “want” to crack. It requires only that the load exceed the structural capacity of the junction that is resisting it.
The energy argument — “the horse would use more energy than their entire diet” — applies to active muscular work, which is not what is being calculated. The passive tensile load on the DDFT during stance is not metabolically expensive in the way that active contraction is. Passive tissue tension requires no ATP. It requires only that the tissue be loaded in the correct anatomical position, which it is, continuously, during every moment of weight-bearing.
The lamellar resistance differential — healthy versus disrupted interdigitation
This is where the argument needs to be made most carefully, because it is the mechanical heart of the matter and it is genuinely underappreciated in online discussions.
In a healthy foot, the lamellar junction provides significant shear resistance to the tendency of P3 to displace relative to the inner hoof wall. The interdigitating dermal and epidermal laminae create a structural bond with a shear strength of approximately 2 MPa across the bonded surface area. The DDFT’s passive tensile load during stance is distributed partly through this junction and partly through the periosteum of P3 and the joint capsule. The junction provides what engineers call a parallel load path — it carries some of the load that would otherwise fall entirely on the DDFT and the bony column.
In a laminitic foot, that parallel load path is disrupted. The basement membrane degrades. The interdigitating laminae lose their structural continuity. The effective shear resistance of the junction falls — in severe cases, to near zero at the dorsal toe, which is the zone of maximum tensile stress and the first region to fail. What replaces the intact lamellar bond in this zone is not structural tissue. It is the lamellar wedge: disorganised fibrous horn and scarred connective tissue that does not interdigitate with the dermis and cannot transfer shear load the way the intact junction does.
The clinical consequence of this is precisely the opposite of what the comment implies. A disrupted lamellar junction does not reduce the mechanical argument for managing DDFT tension — it strengthens it. In the healthy foot, the intact junction shares the load. In the laminitic foot, the junction is not sharing the load at the dorsal toe. Every Newton of DDFT tension that the healthy lamellar junction would have helped resist is now acting against tissue whose structural capacity has been partially or completely lost. The same DDFT tension that the healthy foot tolerated for years is now acting against a degraded structure. That is not a reason to dismiss the forces. It is precisely why the forces matter more in a compromised foot than in a sound one.
“There is no limit on how much heel to trim especially in the first months”
This claim is directly contradicted by the force calculations set out in the article and in Biomechanics for Farriers (Caldwell & Madden, 2025). Each degree of heel drop below the reference DHWA adds approximately 87.5 N of additional DDFT tension in a 500 kg horse — a figure derived from the Eliashar 2004 force plate data and consistent across multiple studies. In a laminitic horse in which the lamellar junction is already compromised, the incremental load applied by an excessive heel reduction in a single session acts against a structure with reduced shear capacity. The 3-degree-per-session guideline is not a conservative preference. It is a biomechanical limit derived from the same force calculations.
The argument that there is no secondary damage to worry about ignores the mechanism entirely. The secondary damage in an over-rapid heel reduction is not visible in the 48 hours following a trim. It accumulates as progressive lamellar separation, increasing founder distance, and worsening rotation — changes that are measurable on serial radiographs weeks later. A horse that walks the following day is not evidence that no tissue damage occurred. It is evidence that the horse’s pain threshold and compensatory mechanisms were not immediately exceeded. Those are not the same thing.
On the clinical case presented in argument
The Friesian case you describe — a horse made recumbent by aggressive trimming, then recovered under your management — is a serious adverse outcome caused by an over-aggressive trim. We do not dispute that aggressive trimming without radiographic guidance causes harm. The article says exactly that. What the article argues is that the solution to aggressive trimming is measured trimming guided by radiographic palmar angle data — not the replacement of one untethered protocol with another.
A horse walking 48 hours after your intervention and ridden at 6 months is a good outcome. That does not validate the claim that there is no limit on heel removal, any more than a horse that survives a road accident validates the claim that speed limits are unnecessary. It validates that you made a good clinical decision in that case. The question is whether the principle — “no limit on heel removal in the first months, no need for radiographs if you are confident” — is safe when applied by every person who reads it in a comment thread and applies it to a different horse with a different palmar angle, a different sole depth, and a different degree of lamellar disruption. That is the standard against which clinical principles should be judged.
On the energy argument and force diagram
The request to produce a force diagram showing the DDFT rotating P3 is reasonable. The diagram in this series does exactly that — it shows the DDFT path, the moment arm at the DIP joint, the GRF vector, and the rotational tendency at the lamellar junction. The force couple is the GRF acting forward of the joint axis through the longer toe lever, and the bony column resisting downward through the joint, with the DDFT tension acting on the solar surface of P3. No head-dropping, triceps engagement, or serratus activation is required for this moment to exist. It exists whenever the GRF acts forward of the joint axis — which, in a horse with a long toe, it does throughout stance.
The energy argument applies to active muscular work. Moment arms and passive structural loading are not metabolically expensive. A long lever on a laminitic foot does not require the horse to expend dietary energy. It requires only geometry.
A final note
The article does not claim that all barefoot trimming is harmful, that no horse has recovered under a non-radiographic protocol, or that every case requires hospital-level intervention. It argues that the published force plate evidence supports specific biomechanical principles, that those principles have measurable clinical consequences, and that protocols which contradict them without radiographic measurement place some horses at risk.
The case you have made here does not disprove the force plate literature. It offers an alternative anatomical framing that contains factual errors, a claim about muscle physiology that misunderstands the difference between active and passive tendon loading, and a clinical case that, by your own account, began with iatrogenic harm caused by exactly the kind of aggressive non-radiographic trimming the article warns against.
We are glad your horse recovered. The argument for measured, radiographically guided care remains unchanged.
References:
Eliashar E, McGuigan MP, Wilson AM. Equine Vet J 2004;36(5):431–435.
Van Heel MCV et al. Equine Vet J 2006;38(3):258–262.
Nominal lamellar shear strength ~2 MPa: Bowker RM et al. cited in O’Grady SE, Parks AH. Vet Clin North Am Equine Pract 2003;19(2):393–416.