
Suspensory Desmopathy in Horses
Chronic Proximal Suspensory Ligament Desmopathy in Horses: Biomechanics, Postural Adaptation, Hoof Capsule Morphology, and Treatment Strategies
Caldwell M. N. Scientific Horseshoeing, 116, Newcastle Road, Talke, Staffordshire. ST7 1SA. Email info@hoofflix.com
1. Introduction
Chronic desmopathy of the proximal suspensory ligament (PSL), particularly in the hindlimb, is a well-recognized cause of persistent performance limitation and lameness in equine athletes. The PSL plays a critical role in metatarsophalangeal joint support, contributing to elastic energy storage and the control of fetlock extension during locomotion [Gillis et al., 1995; Robert et al., 2001]. When subjected to chronic overload, particularly from abnormal limb posture or biomechanical compromise, the PSL undergoes structural degeneration and fibrosis, culminating in clinical desmopathy.
Recent insights underscore the importance of hoof capsule morphology, neuromuscular compensation, and postural pain avoidance as interrelated contributors to the pathogenesis and perpetuation of this condition.
2. Functional Anatomy and Mechanical Loading of the PSL
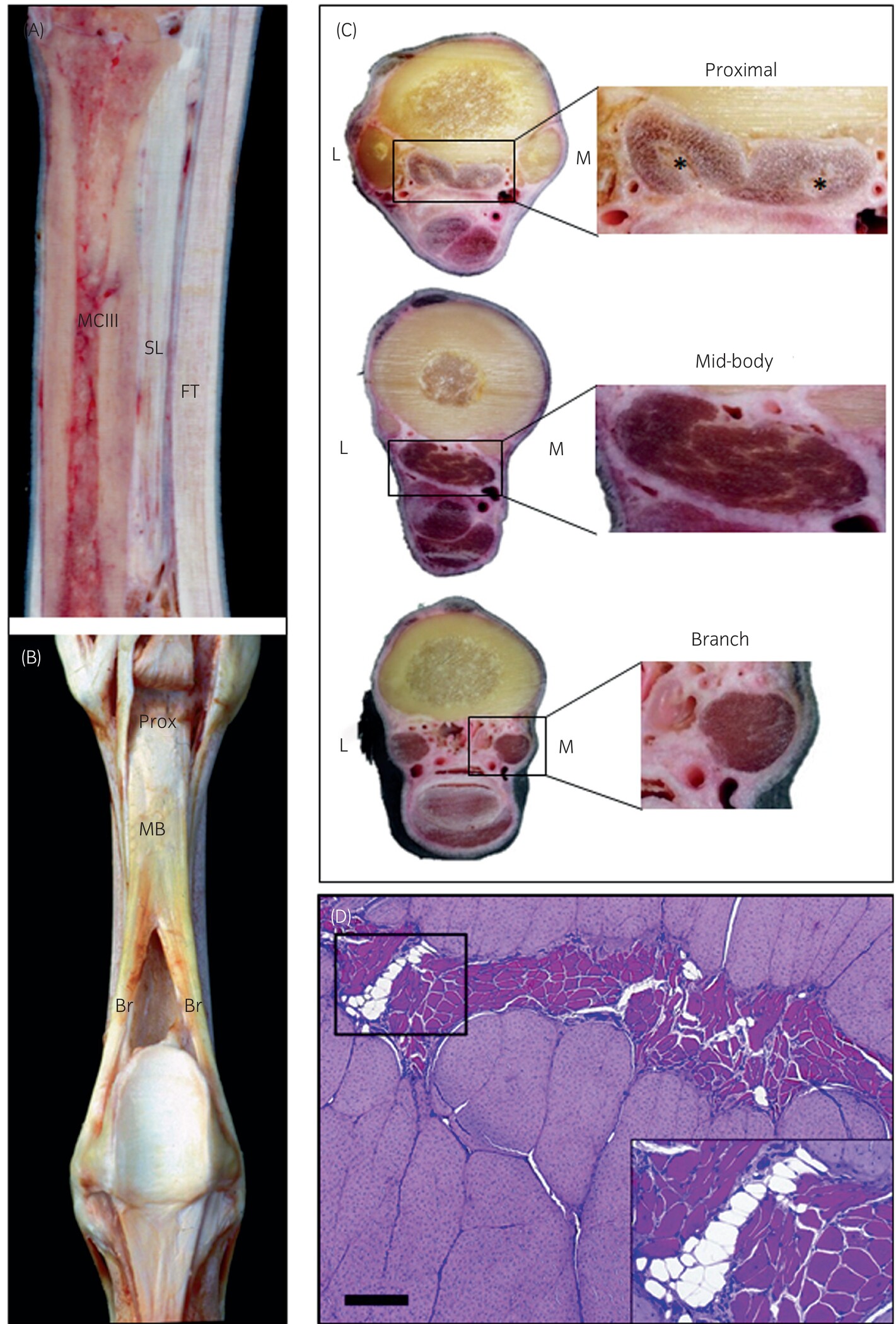
In the hindlimb, the PSL originates from the proximoplantar aspect of the third metatarsal bone, coursing between the splint bones before branching to the proximal sesamoids. Its anatomical positioning—deep within the tarsal canal and against the palmar cortex—predisposes it to compressive and tensile stress when limb mechanics are altered, particularly in horses with upright hock conformation or caudally shifted loading patterns [Dyson et al., 2008].
The suspensory ligament’s primary function is to resist excessive fetlock extension and absorb energy during midstance. Chronic overstrain, especially in a horse with poor sagittal hoof balance (long toe–low heel or negative plantar angle), increases mechanical load at the origin, risking microtrauma and eventual ligament degeneration [Denoix et al., 2014; Sharp, 2022].
3. Hoof Capsule Morphology and Negative Plantar Angle
Negative plantar angle (NPA) describes a hind hoof orientation in which the solar surface of the hoof is lower at the heel than the toe, often due to underrun or collapsed heels. This morphology alters the vector of ground reaction force (GRF)and encourages a hyperextended digit at midstance, shifting the mechanical burden proximally toward the suspensory ligament origin [Turner, 2003].
Sharp (2022) demonstrated that altering the dorso-plantar hoof balance can measurably affect hindlimb posture and limb orientation, supporting the theory that hoof morphology contributes to chronic PSL loading. Moreover, poor hoof conformation often coexists with compensatory pelvic tilt, stifle flexion, or hip retraction, which can further exacerbate PSL stress through altered kinetic chain dynamics.
4. Postural Adaptation and Pain Avoidance Strategies
Horses experiencing proximal suspensory pain often exhibit chronic postural compensations as a form of biomechanical self-protection. This includes:
Pelvic tucking or tilting (anterior or lateral)
Asymmetric weight shifting
Hind limb abduction or adduction (base-narrow or base-wide)
Canted-in stifles
Toe-dragging and shortened cranial phase of the stride
These postural shifts serve to reduce mechanical load on the affected suspensory region but result in altered limb dynamics, which have downstream effects on hoof capsule morphology.
Over time, chronic compensation leads to:
Medio-lateral imbalance of the hoof capsule due to asymmetric limb loading
Distorted horn tubule growth, especially in the heel quarters
Flattening or underrun of the plantar surface, especially where toe-first landing is adopted
Development of asymmetrical frogs and bars, correlating with habitual stance and loading vectors
These hoof distortions, in turn, perpetuate the abnormal mechanical environment, reinforcing the pathomechanical loop of PSL desmopathy.
5. Gait Dynamics and Neuromuscular Reorganization
Quantitative gait analysis of horses with hindlimb suspensory pathology has revealed several consistent patterns:
Reduced fetlock drop at midstance, suggesting unloading of the suspensory mechanism
Delayed or reduced hock flexion
Increased pelvic pitch asymmetry
Altered vertical force and propulsion vectors during hindlimb stance phase [Pfau et al., 2007; van Weeren & Pfau, 2018]
These changes reflect neuromuscular reorganization—the horse’s nervous system adapting movement patterns to avoid nociceptive stimuli from the damaged ligament. While adaptive in the short term, this results in chronic compensation and overload of secondary structures, including the deep digital flexor tendon, lumbosacral musculature, and gluteal stabilizers.
6. Diagnosis and Imaging
Chronic PSL desmopathy often requires:
Local diagnostic analgesia of the deep branch of the lateral plantar nerve
Ultrasonographic evaluation for fiber disruption, echogenicity loss, and periligamentous fibrosis
MRI for detection of osseous edema at the PSL origin and subtle chronic lesions
Gait analysis, including inertial sensors or video vector tracking, to quantify asymmetries and limb positioning
7. Treatment Strategies
7.1 Conservative and Regenerative Therapy
Rest and structured rehabilitation, especially in early or mild cases
Extracorporeal shockwave therapy (ESWT) to promote neovascularization [Witte et al., 2004]
Biologics: Platelet-rich plasma (PRP), stem cells, or IRAP for ligament healing [Geburek et al., 2015]
NSAIDs, physiotherapy, and lumbosacral mobilization
7.2 Surgical Management
Plantar fasciotomy and neurectomy (PFN) of the lateral plantar nerve: Reduces chronic pain in refractory cases [Schramme et al., 2010]
7.3 Therapeutic Farriery
The goal of farriery is to correct the biomechanical environment, particularly by:
Elevating the plantar angle (via wedges, heel platforms, or graduated shoes)
Reducing digital hyperextension and hence load at the PSL origin
Optimizing breakover and caudal support
Addressing mediolateral imbalances to reduce torque
Incorporating frog support or bar shoes in horses with collapsed heels
Dynamic shoeing protocols should be guided by radiographs, gait analysis, and ongoing postural observation, with frequent reassessment and gradual tapering.
8. Conclusion
Chronic PSL desmopathy represents not just a localized ligament injury but a whole-body biomechanical dysfunction, often initiated or perpetuated by poor hoof morphology and sustained through pain-driven postural adaptation. Understanding the feedback loop between ligament injury, limb dynamics, and hoof capsule distortion is essential for effective, multidisciplinary management. A combination of targeted farriery, biologic therapy, and neuromuscular rehabilitation is likely to offer the best long-term prognosis.
9. References
Dyson, S. et al. (2008). Proximal suspensory desmitis: clinical features and diagnosis. Equine Vet J, 40(S36): 36–41.
Gillis, C.L., et al. (1995). The functional anatomy of the equine suspensory apparatus. Equine Vet J, 27(5): 333–337.
Sharp, Y. (2022). Effects of Changing Dorso-Plantar Hoof Balance on Equine Hind Limb Posture. Animals, 12(23): 3275.
Denoix, J.M., et al. (2014). Ultrasound anatomy and pathology of the proximal suspensory ligament. Vet Clin Equine, 30(1): 1–21.
Pfau, T., et al. (2007). Temporal and spatial gait asymmetries in horses with suspensory ligament desmitis. Equine Vet J, 39(3): 256–261.
Turner, T.A. (2003). Therapeutic shoeing for hind limb suspensory desmitis. AAEP Proc, 49: 197–199.
van Weeren, P.R. & Pfau, T. (2018). Gait analysis in the horse: History, challenges, and future directions. Equine Vet J, 50(5): 564–568.
Schramme, M.C., et al. (2010). Surgical management of chronic hindlimb proximal suspensory desmopathy. Equine Vet J, 42(4): 317–323.
Witte, S., et al. (2004). Shockwave therapy for suspensory desmitis. Vet Rec, 154(9): 274–278.
Geburek, F., et al. (2015). Intra‐ligament injections of platelet concentrate in chronic suspensory ligament disease. Equine Vet J, 48(2): 185–193.
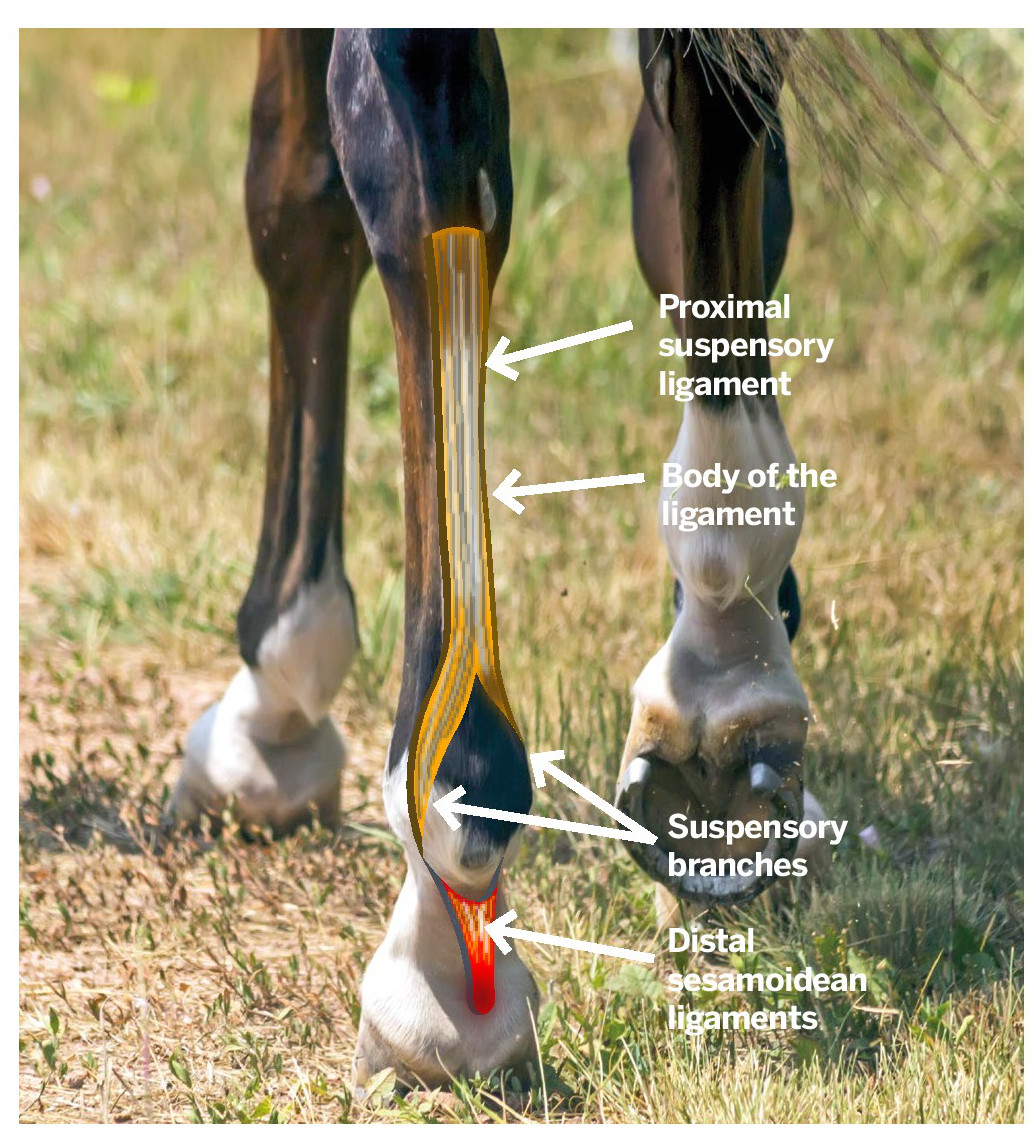
Visual representation of the SL



Duo eclipse elevated bar shoe used by the author in acute cases DPSL injuries