")
Low Ringbone: Understanding and Managing Distal Interphalangeal Joint Osteoarthritis
A practical science summary for horse owners and equine professionals — covering diagnosis, biomechanics, and the full spectrum of farriery options from rolled toe to full roller-motion shoe.
Low ringbone, the clinical shorthand for distal interphalangeal (DIP) joint osteoarthritis, is one of the most consequential diagnoses in the sport horse. It is progressive, it is common in warmbloods and heavy-bodied horses, and it demands a coordinated response from vet and farrier working from the same diagnostic information. This article distils the key science into a practical overview.
What Is DIP Joint Osteoarthritis?
The DIP joint — the articulation between the short pastern bone (P2) and the coffin bone (P3) — undergoes 10 to 15 degrees of flexion and extension with every stride. During that cycle, it is exposed to substantial compressive, shear, and torsional forces that increase sharply at speed, during jumping, and in collected dressage work.
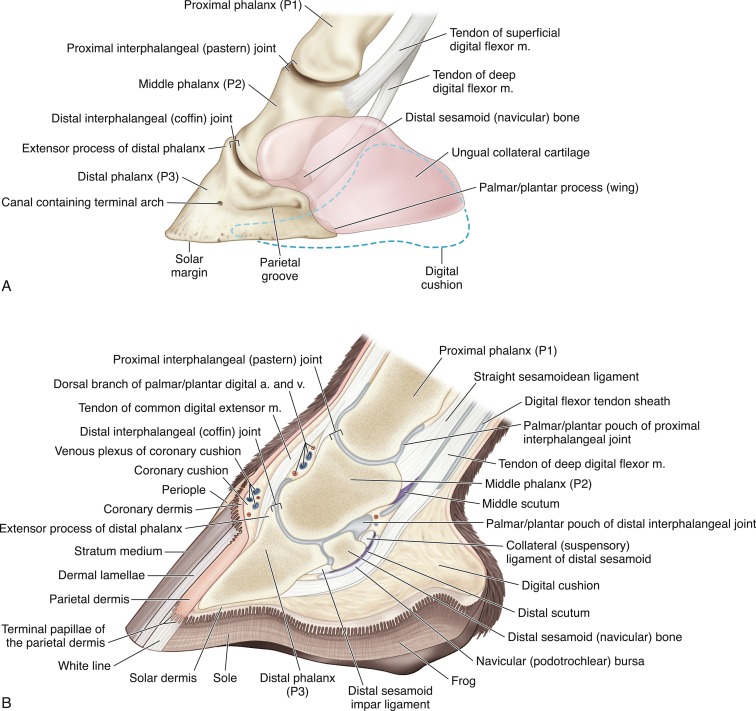
Fig 1. Detailed anatomy of the equine foot. Note the complexity of anatomical structures in and around the Distal Interphalangeal Joint (DIPJ).
Osteoarthritis of this joint — low ringbone — is characterised by the gradual loss of articular cartilage, the formation of bony spurs (osteophytes) at joint margins, fibrosis of the joint capsule, and sclerosis of the underlying bone. In advanced cases, this bony proliferation can be felt and sometimes seen at the coronary band, forming the visible “ring” that gives the condition its name.
Clinicians distinguish two forms:
- Articular ringbone — involves the joint surfaces directly and carries a more guarded prognosis.
- Periarticular (non-articular) ringbone — bony proliferation at the margins without direct cartilage involvement, which may produce relatively mild lameness.
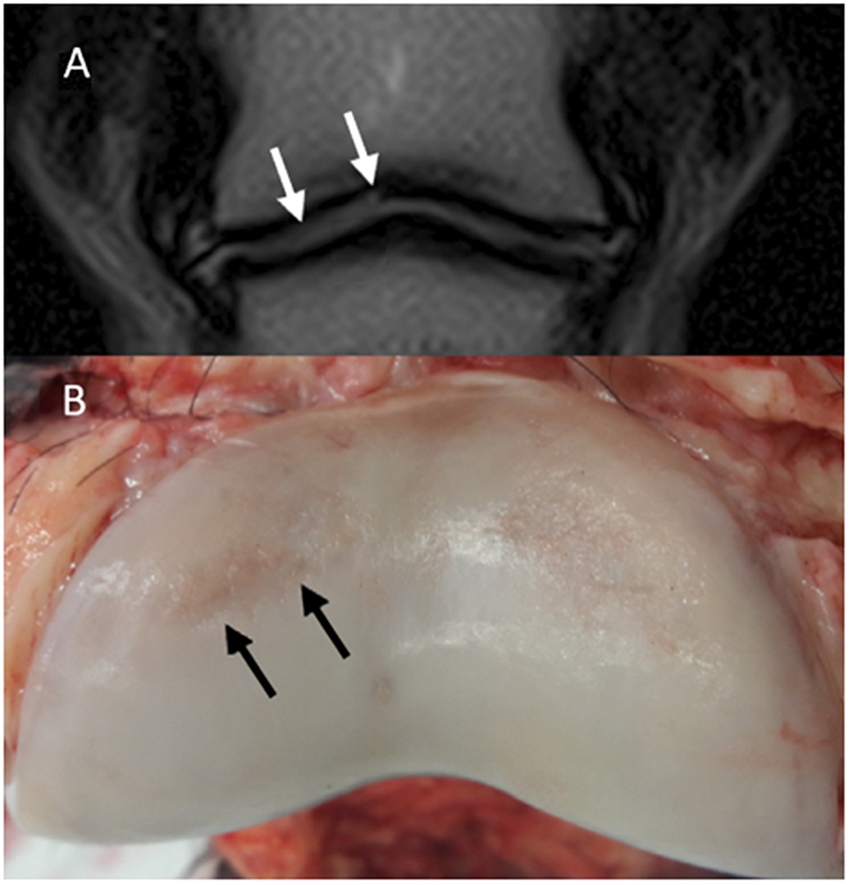
Fig 2. Magnetic resonance (MR) and macroscopic images of the same horse. Lateral is to the left; (A) Dorsal T2-weighted FSE. A hyperintensity is noted in the lateral aspect of the articular cartilage of the middle phalanx (P2) (white arrows). (B) Gross appearance of P2. There are cartilage erosions in the dorsolateral (black arrows) and dorsomedial aspects of the articular surface. The cartilage defect on the dorsomedial aspect appears more superficial compared to the dorsolateral aspect and could not be identified in MR images.
How Does It Present?
The classic presentation is a bilateral forelimb lameness with a stiff, stilted quality — worse after rest and transiently better after warming up. Owners often notice toe-dragging, reluctance at canter transitions, shortened stride, and unwillingness to engage in collected work. Visible swelling at the coronary band is a late sign; the confined space within the hoof capsule masks effusion until disease is advanced.
Diagnosis is confirmed by the combination of positive distal limb flexion, a positive response to intra-articular DIP joint local anaesthesia (the gold standard for identifying the joint as the primary pain source), and radiographic changes. MRI adds important detail on cartilage thickness, bone marrow oedema, and any concurrent deep digital flexor tendon or collateral ligament pathology — all of which influence the farriery prescription.

Fig. 3. For the dorsal perpendicular approach to the DIP joint, the needle is inserted at the proximal edge of the coronet, approximately 0.75 inch ( 2 cm) lateral or medial to the midpoint of the coronet (ie, at the edge of the extensor ligament). The needle is directed distally, perpendicular to the bearing surface of the hoof.
Why Does It Develop? Key Risk Factors
- Long-toe low-heel conformation — extends the lever arm (moment arm) acting on the DIP joint at each breakover. Even a single centimetre of excess toe length meaningfully increases DIP joint loading.
- Mediolateral imbalance — asymmetric loading creates shear forces that accelerate cartilage wear on the overloaded compartment.
- Toe-in / toe-out deviation — rotates the breakover axis off the sagittal plane, imposing torsional (rotational) loading on the joint at every stride.
- Athletic discipline — dressage collection demands sustained DIP joint flexion under load; cross-country landing generates peak compressive forces.
- Breed and body mass — heavy-bodied warmbloods with relatively small feet generate high compressive force per unit area at the joint surface.
The Biomechanics: What Farriery Is Actually Doing
Three biomechanical principles guide every farriery decision in DIP OA:
1. Reducing the extension moment arm
The extension moment acting on the DIP joint equals the ground reaction force (GRF) multiplied by the perpendicular distance from the joint axis to the breakover point. Moving breakover palmarly by any means shortens this moment arm and directly reduces stress at the joint. This is the theoretical basis for all breakover modification.
2. Redistributing GRF through the solar surface
On a standard sharp-toe shoe, the GRF during the final phase of stance concentrates force at the dorsal toe edge — the most degenerate region of the DIP joint precisely when the peak extension moment is applied. A perimeter bevel (at the toe alone, across the quarters, or around the full shoe) shifts the effective contact point proximally and distributes the exit loading more broadly. Aoun et al. (PeerJ, 2025) confirmed in instrumented trials that a 45-degree perimeter bevel on the shoe reduces limb loading rate and produces smoother GRF patterns through stance compared to a standard perimeter shoe.
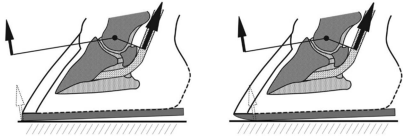
fig 4. The extension moment acting on the DIP joint equals the ground reaction force.
3. Reducing torsional loading from off-axis breakover
A standard rolled toe corrects the sagittal breakover but leaves the rotational component unchanged in a horse with toe-in or toe-out deviation. Extending the bevel around the lateral quarter (toe-in foot) or medial quarter (toe-out foot) allows the foot to escape in its actual direction of travel, removing the torsional resistance at the hoof-ground interface and reducing capsular torque at the DIP joint with every stride.

Fig 5. A standard rolled toe corrects the sagittal breakover
The Farriery Options: A Practical Spectrum
There is no single correct shoe for DIP OA. The appropriate option depends on disease severity, mediolateral symmetry, the horse’s conformational deviation, and the work demands. The following represents the progression from simplest to most comprehensive:
| Shoe Option | Best Used When | Key Limitation |
| Rolled Toe | Early OA; good mediolateral balance; no significant deviation | Does not address off-axis or asymmetric loading |
| Rolled Toe + Partial Quarter Bevel | Any horse with consistent toe-in or toe-out deviation | Bevel side must match deviation; requires careful assessment |
| Full Roller-Motion (Perimeter Bevel) | Advanced or bilateral OA; variable breakover pattern; multi-directional protection needed | Not ideal if heels are severely underrun — partial bevel preferred |
| COR-Centred + Quarter Bevel | Performance horse where precise moment arm reduction is critical; consistent deviation | Requires radiographic COR fitting not a field-side option |
| Wide-Web + Full Bevel + Pour-in Composite | Advanced OA with reduced sole depth; horses in hard-surface work | Increased weight prefer aluminium; not suitable for racing |
The Trimming Foundation
No shoe can compensate for poor trim. The three trimming priorities for DIP OA, in order of importance, are:
- Mediolateral balance equal heel heights and symmetric wall heights; the DIP joint should be balanced on the dorsopalmar radiograph.
- Hoof-pastern axis correction toward neutral primarily through trimming, not heel elevation. Where confirmed cartilage loss exists, heel elevation above 2 degrees is contraindicated as it shifts compressive load to the already-compromised dorsal compartment.
- Toe length minimised maintaining at least 15 mm of sole depth above P3.

Fig 6. Geometric proportions and medio lateral hoof balance form the basis of any farriery management protocol.
A practical tip: before removing the old shoe, examine the wear pattern. Pronounced wear on the lateral toe in a toe-in horse confirms the laterally displaced breakover axis and tells the farrier precisely where the quarter bevel should sit on the new shoe.

Fig 7. Asymmetrical shoe wear can be an indicator of pathology
Veterinary Management: The Medical Side
Farriery and veterinary management are complementary, not alternatives. The standard medical pathway includes intra-articular corticosteroids (triamcinolone acetonide at 3-to-6-month intervals; methylprednisolone acetate for longer duration), hyaluronic acid, and biologics such as PRP or IRAP for horses where steroid frequency is a concern. Bisphosphonates (tiludronate, clodronate) are indicated when subchondral bone remodelling is the predominant radiographic finding. NSAIDs provide analgesic support during acute flares.
Surgical arthrodesis fusion of the DIP joint is reserved for horses with severe bilateral OA refractory to all conservative management. It is technically demanding and less commonly performed than pastern joint arthrodesis.
Fig 8. The standard medical pathway includes intra-articular corticosteroids (triamcinolone acetonide at 3-to-6-month intervals; methylprednisolone acetate for longer duration), hyaluronic acid, and biologics such as PRP or IRAP for horses where steroid frequency is a concern.
Monitoring, Progression, and Owner Expectations
DIP OA is progressive. The shoe that works well at initial fitting will become less effective as cartilage loss advances the farriery prescription must evolve with the disease. A brief lameness assessment before each trim, documented at 4-week intervals, provides the longitudinal record that guides the next decision. Annual radiographic review recalibrates the approach to current structural status.
If lameness has not improved within 8 weeks after a well-considered shoe change, the differential is straightforward: the shoe was incorrectly specified, the diagnosis is incomplete, or concurrent medical management is insufficient. Any of those is correctable but only if the team is communicating and documenting.
Owner counselling must establish from the outset that farriery improves comfort and slows progression — but it does not restore cartilage. The goal is a horse that remains comfortable and functional in appropriate work for as long as possible.
Key Takeaways
- Mediolateral balance is the single most important trimming objective more important than breakover modification.
- Rolled toe is the correct starting point for early DIP OA with no deviation but it is incomplete if off-axis loading is present.
- A partial quarter bevel matched to the horse’s actual swing axis reduces torsional loading at each stride a modification that standard rolled-toe management misses.
- The full roller-motion shoe provides multi-directional breakover protection and is supported by both biomechanical study (Aoun et al., 2025) and substantial clinical experience for articular OA.
- For advanced OA with compromised solar depth, a wide-web full roller-motion shoe with pour-in composite offers the most comprehensive protection available for a horse remaining in work.
- The farriery prescription must evolve as the disease progresses — annual radiographic review and documented lameness monitoring are non-negotiable.
**This article is based on clinical and scientific literature including Aoun et al. (PeerJ, 2025), Van Heel et al. (2006), and O’Grady & Steward (2003, 2007). Evidence grades are indicated in the source material: [CS] = controlled study; [EX] = expert consensus. Content is intended for educational purposes and does not replace veterinary or farriery assessment of individual horses.