
Is dorsal hoof wall resection a misunderstood and under-used hoof capsule management tool in equine laminitis?
Mark N Caldwell., PhD., FWCF
Scientific Horseshoeing & HoofFlix. TV
Correspondence: info@hoofflix.com
Word count (excluding references and abstract): ~5,200
Keywords:
Equine laminitis; dorsal hoof wall resection; hoof capsule management; lamellar pathology; founder; farriery; biomechanics
Abstract
Dorsal hoof wall (DHW) resection has been advocated in the treatment of laminitis for over forty years, yet its role remains contentious and underutilised. This review summarises the anatomical and physiological changes occurring within the equine foot from the onset of acute laminitis through the transitional stage to chronic founder, and considers the biomechanical and pathophysiological rationale for DHW resection. The hypothesis that resection relieves dorsal hydraulic pressure, improves perfusion, reduces pain, and prevents catastrophic laminar failure is explored. Particular emphasis is placed on its potential role during the transition between acute and chronic disease, where early decompression may alter prognosis. In chronic founder, the technique may also aid management of lamellar hyperplasia and dysplastic horn production. Criteria and technique, as first outlined by Eustace and Caldwell (1989), are described in detail, alongside clinical evidence. The importance of accurate diagnostic imaging and timely intervention is stressed, as these non-invasive procedures may reduce pain and support more effective healing. While high-quality prospective evidence remains limited, DHW resection deserves renewed attention as a hoof capsule management tool in the multidisciplinary treatment of equine laminitis.
Introduction
Equine laminitis is a complex, multifactorial disease with devastating consequences for welfare and performance. Its hallmark is structural and functional failure of the suspensory apparatus of the distal phalanx (P3), which is normally suspended within the hoof capsule by the interdigitation of epidermal and dermal lamellae anchored to a basement membrane (Pollitt, 1996). The dorsal lamellae bear particularly high mechanical loads during breakover, further magnified by the pull of the deep digital flexor tendon (McGuigan & Wilson, 2001).
DHW resection, the surgical removal of a segment of the dorsal hoof wall, was introduced clinically to relieve pressure, drain submural exudate, and eliminate necrotic wall tissue (Eustace & Caldwell, 1989). Although promising results were reported, the technique remains variably applied and often regarded as a last-resort intervention (Colles, 1991). This reluctance may in part stem from misunderstanding of its rationale, uncertainty about technique, and fear of destabilising the hoof capsule.
This review revisits the anatomical and physiological basis for DHW resection, situating the technique within the laminitic timeline and examining its potential as an early, non-invasive adjunct to improve outcomes.
The laminitic timeline
Acute onset (0–48 hours):
The acute stage is characterised by inflammatory activation, vascular dysfunction, and basement membrane failure (Belknap et al., 2007; Pollitt, 1996; Pollitt et al., 2004). Histological studies demonstrate stretching and separation of secondary epidermal lamellae. In endocrinopathic laminitis, vascular dysregulation produces oedema within the non-compliant hoof capsule (de Laat et al., 2016).
Transitional stage (2–7 days):
Clinical lameness persists, but overt inflammatory markers diminish. The lamellae remain elongated, weakened, and susceptible to mechanical displacement. P3 rotation is driven by the persistent strain of the DDFT acting against compromised dorsal lamellae (Karikoski et al., 2014). This is a critical stage where interventions to relieve dorsal pressure and support capsule realignment may alter prognosis.
Chronic founder (>4 weeks):
Once displacement occurs, maladaptive tissue responses dominate. A lamellar wedge of dysplastic horn develops between the dorsal wall and P3, perpetuating malalignment and preventing reattachment. Osteolysis of P3 may also ensue (Rucker, 2010).
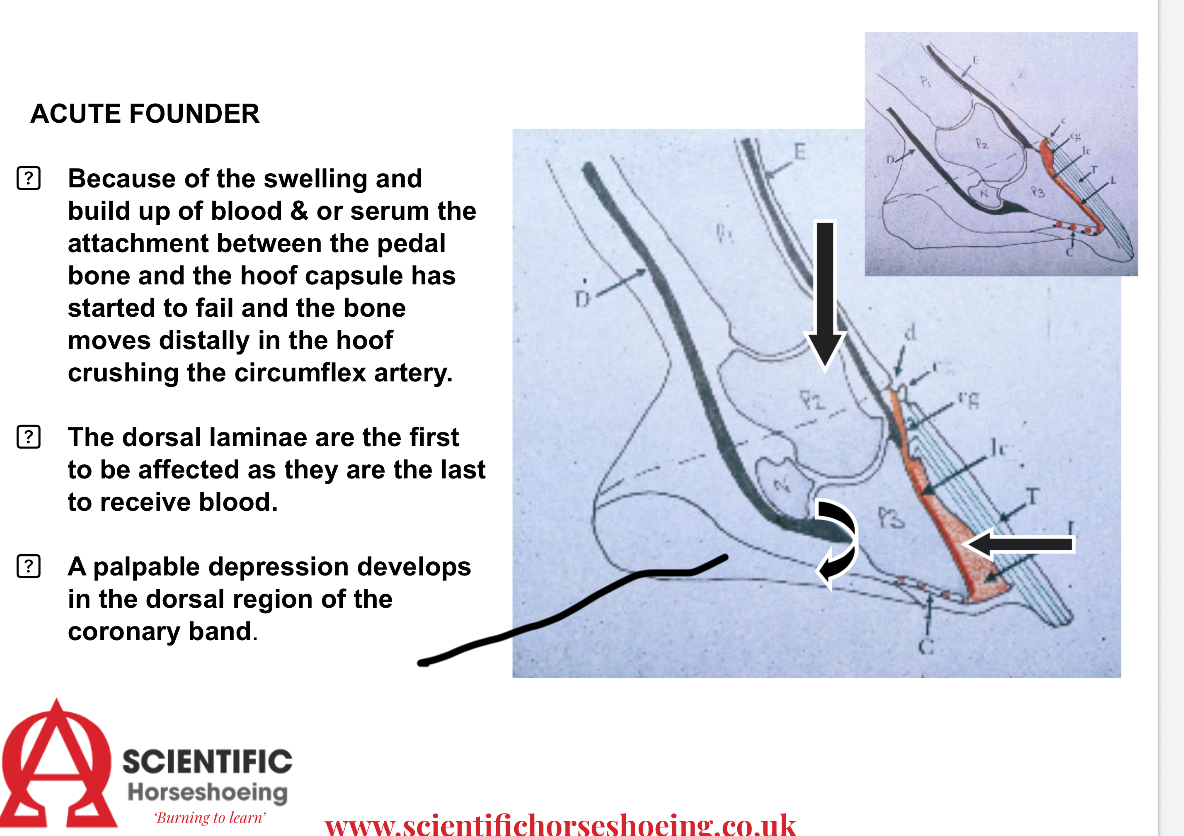
Figure 1: Schematic illustration of the lamellar interface in health (left), acute laminitis with basement membrane separation and oedema (centre), and chronic founder with lamellar wedge formation and distal phalanx rotation (right).
Biomechanical rationale for dorsal hoof wall resection
The hoof capsule acts as a rigid shell. In acute and transitional laminitis, the accumulation of serum exudate and lamellar oedema beneath the dorsal wall creates a closed, high-pressure compartment. This pressure compromises perfusion and exacerbates pain, much like a compartment syndrome. Resection provides decompression, permitting drainage and improved circulation. Clinicians have reported rapid pain relief and improved stance following the procedure, although controlled studies remain limited.
From a mechanical perspective, removing non-functional wall tissue eliminates a pathological lever at the toe, allowing more effective realignment trimming and shoeing strategies such as breakover reduction and frog/sole support (Witte et al., 2023). This in turn reduces shear on the damaged lamellae and stabilises P3.
Figure 2: Diagram showing hoof loading pathways: (A) healthy foot with balanced load transfer via lamellae; (B) laminitic foot with excessive dorsal wall tension and displacement forces; (C) post-resection foot with reduced dorsal tension and improved mechanical alignment. (Photo credit Patrick Reily)
Criteria and technique for resection
Eustace and Caldwell (1989) set out clinical criteria for resection. Indications include solar prolapse, undermined or non-viable dorsal wall, and the presence of submural exudate or abscessation. Persistent pain localised to the dorsal wall despite systemic therapy also justifies consideration.
The technique involves removing a vertical strip of the dorsal wall from the coronary band to the ground surface over the affected area. The resection tapers proximally to preserve coronary horn growth. Only the compromised wall and non-viable lamellar horn are removed, avoiding unnecessary trauma to sensitive structures. A heart-bar shoe is applied to redistribute load towards the heels and frog, stabilising P3 during recovery. The exposed lamellae are protected with sterile dressings to support horn regrowth.

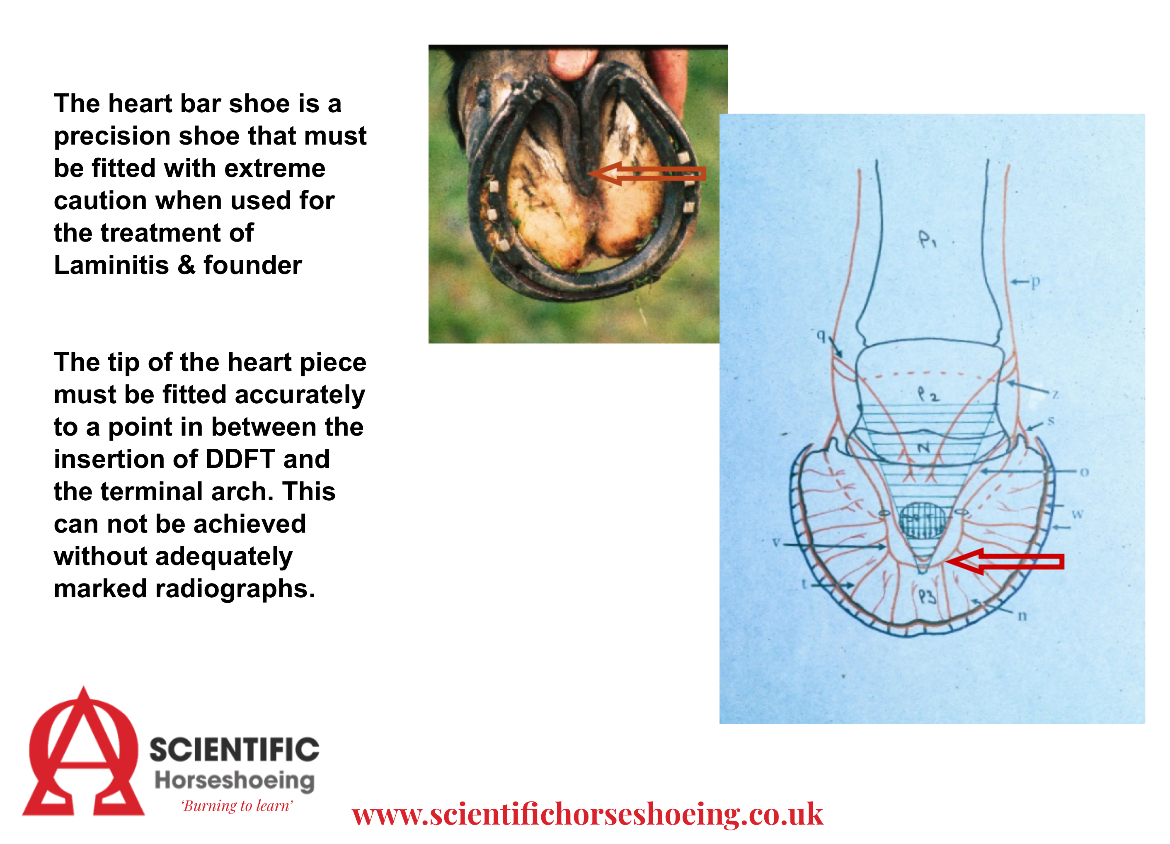
Figure 3: Stepwise illustration of the dorsal hoof wall resection technique: (A) pre-operative hoof capsule with dorsal distortion; (B) resection window prepared with removal of non-viable wall; (C) application of heart-bar shoe with frog support; (D) schematic considerations for correct fitting of a heart-bar shoe to prohibit vascular occlusion.
Application in acute and transitional laminitis
The greatest potential benefit of DHW resection may lie in the transitional stage. At this point, lamellae remain weak but salvageable. Decompression and pain relief may reduce abnormal stance adaptations, thereby lowering DDFT tension and preventing further displacement. When combined with realignment trimming and appropriate support, the technique offers a non-invasive adjunct aimed at preventing catastrophic laminar failure.
Application in chronic founder
In chronic cases, the lamellar wedge represents a pathological barrier to capsule realignment. Strategic resection of this wedge removes dysplastic horn and creates space for new coronary horn to grow in a corrected trajectory. Combined with realignment shoeing, this can improve coupling between P3 and the dorsal wall, potentially improving long-term soundness (Rucker, 2010).

Figure 4: (A) chronic founder with lamellar wedge displacing the dorsal wall; (B) post-resection foot showing removal of dysplastic horn and corrected alignment pathway for new wall growth.
Diagnostic imaging and clinical assessment
Central to the safe and effective use of DHW resection is accurate, high-quality diagnostic imaging. Radiography provides essential information on P3 position, capsular distortion, and lamellar wedge dimensions, guiding the extent and placement of resection. Advanced imaging modalities, including venography, may help identify perfusion deficits that justify decompression. Clinical assessment of digital pulses, hoof capsule heat, and pain response remain equally important. Timely recognition of transition to displacement is crucial, as DHW resection at this point may influence prognosis.
Risks, contraindications, and aftercare
Resection is contraindicated in horses with generalised “sinkers,” where global capsular instability precludes benefit. Excessive or poorly planned resection risks destabilisation and infection. Aftercare is vital: exposed lamellae must be protected with sterile dressings, and long-term support shoeing maintained. When performed conservatively, in suitable cases, with meticulous aftercare, DHW resection is safe and minimally invasive.
Discussion and conclusion
Dorsal hoof wall resection is a technique that has been misunderstood and, as a result, under-used in modern laminitis management. While sometimes regarded as a desperate measure, the pathophysiological rationale suggests it may be most valuable during the transition between acute and chronic disease, when early decompression could reduce pain, improve perfusion, and limit displacement. In chronic founder, resection offers a means of controlling lamellar hyperplasia and creating conditions for more functional hoof capsule regrowth.
Critically, DHW resection should never be viewed as a stand-alone procedure. Its success depends on accurate diagnostic imaging, careful case selection, and integration with realignment farriery and systemic disease management. With these safeguards, it represents a non-invasive, biologically rational adjunct to reduce pain and improve prognosis.
Further research is needed to quantify its effects on intralaminar pressure, perfusion, and long-term outcomes. In the meantime, DHW resection deserves reconsideration as a practical, evidence-informed tool that can improve prognosis when applied judiciously.
for more information subscribe and follow our series the laminitis debate.https://hoofflix.com/media/videos/anatomy-of-lower-limb-and-foot/laminitis-the-big-debate-hosted-by-neil-madden-fwcf/
References
Belknap, J.K., Giguère, S., Pettigrew, A., Cochran, A.M., van Eps, A.W. & Pollitt, C.C. (2007) Lamellar pro-inflammatory cytokine expression in the carbohydrate overload model of equine laminitis. Equine Veterinary Journal, 39(3), 241–247.
Colles, C.M. (1991) Laminitis in the pony: conservative treatment versus dorsal hoof wall resection. Equine Veterinary Journal, 23(4), 243–246.
de Laat, M.A., Sillence, M.N., McGree, J.M. & Pollitt, C.C. (2016) Vascular dysfunction in horses with endocrinopathic laminitis. Frontiers in Endocrinology, 7, 39.
Eustace, R.A. & Caldwell, M.N. (1989) Treatment of solar prolapse using the heart bar shoe and dorsal hoof wall resection technique. Equine Veterinary Journal, 21(5), 370–372.
Karikoski, N.P., Horn, I., McGowan, C.M. & Asplin, K.E. (2014) Pathology of natural cases of equine endocrinopathic laminitis associated with hyperinsulinaemia. Veterinary Pathology, 51(6), 1279–1292.
McGuigan, M.P. & Wilson, A.M. (2001) The effect of gait and digital flexor muscle activation on limb compliance in the forelimb of the horse. Journal of Experimental Biology, 204, 3979–3990.
Pollitt, C.C. (1996) Basement membrane pathology: a feature of acute equine laminitis. Equine Veterinary Journal, 28(1), 38–46.
Pollitt, C.C., Pass, M.A., Pollitt, S. & Kyaw-Tanner, M. (2004) Cleavage of laminin-5 associated with basement membrane pathology in equine laminitis. Equine Veterinary Journal, 36(3), 230–235.
Rucker, A. (2010) The lamellar wedge. Veterinary Clinics of North America: Equine Practice, 26(1), 179–195.
van Eps, A.W. & Pollitt, C.C. (2011) Equine laminitis: cryotherapy reduces the severity of the acute lesion. Equine Veterinary Journal, 43(6), 739–744.
Witte, S., Wilson, A.M., Pfau, T. & Wakeling, J.M. (2023) Shoe configuration effects on third phalanx and capsule motion of equine hooves with and without laminitis. Veterinary and Comparative Orthopaedics and Traumatology, 36(5), 255–265.