
Inside the Lamanitic Hoof.
An Investigative Look at Dr. Ric Redden’s Approach to Chronic Laminitis
By Mark Caldwell, PhD FWCF
Prologue – The Case That Changed Everything
Imagine a farriery clinic where veterinarians and farriers work side by side, reviewing radiographs and venograms in real time over Skype. That’s the world Ric Redden has built—an investigative podiatry practice treating horses deemed beyond hope. His consulting service, where he works through each case step-by-step remotely, is renowned for turning around “hopeless” chronic laminitis cases.
As I explore his work, I hear questions echoing in every reader’s mind: How does he diagnose what others miss? What mechanical science underpins his protocol? When does he reach for surgery? And why do his results differ so strongly from standard farriery?
Why Venograms? Redden’s Answer Unpacked
Q: What’s wrong with X-rays alone?
Redden says radiographs show bone alignment but not blood flow. Horses that look stable externally may have ventral lamellar sections devoid of perfusion. It’s here that venograms—taken while the horse stands—make the difference. He has performed well over 3,000 digital venograms, identifying perfusion deficits unseen on X-rays, and correlating recovery with vascular improvement ([turn0search6]; [turn0search4])NANRICveterinaryevidence.org.
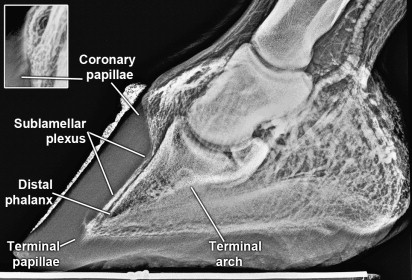
Fig. 1 Venogram of the normal, sound foot of a 400-kg American quarter horse. The coronary (inset), terminal, and solar papillae are oriented in the same plane as the dorsal face of the distal phalanx (DP). The sublamellar-circumflex junction is at a sharp 50° angle, similar to that of the DP’s apex.

Fig. 2. The venogram of the foot of a horse with peracute, severe distal displacement (sinker) of the DP, 2 weeks after contralateral limb injury. The pathology is extensive, and the entire dorsal foot is void of contrast. Vessels are truncated at the coronary band with minimal contrast in the terminal arch and heel. This horse was euthanised.
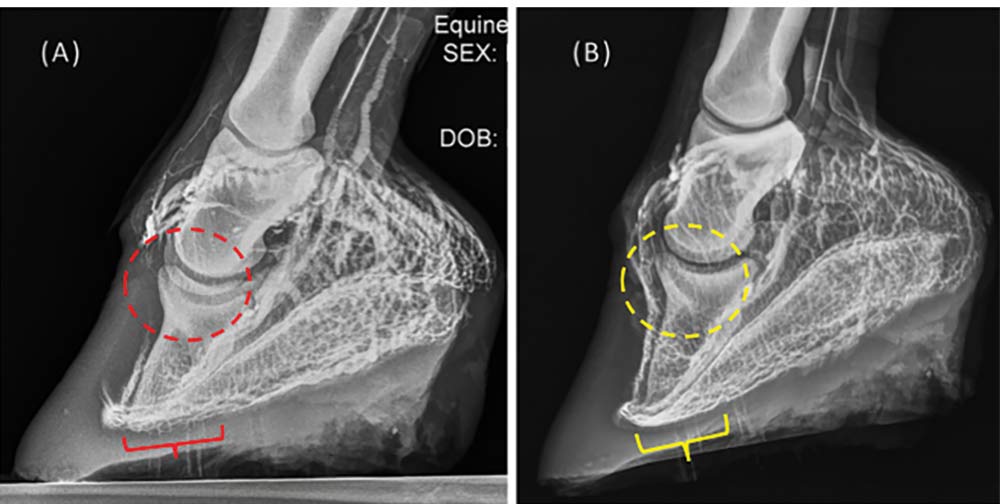
Fig 3. A) occlusion of the coronary arterial plexus and circumflex arteries and B) re perfusion during unloading.
Q: How exactly are they done?
Redden’s technique is precise: use a tourniquet at the fetlock, inject contrast dye into the digital vein, and capture imaging at the 30–45 second mark. Foot position must be block-level, x-ray beam horizontal and at frog height, with visible wall markers to locate exact anatomy.

fig 4. Performing digital venography.
What Defines Laminitis in Redden’s World?
Redden’s model combines two astrophs of pathological change:
Vascular failure — especially in dorsal lamellae.
Mechanical collapse — where GRF and DDFT tension cause P3 rotation or vertical sinking.
He argues that vascular loss is the trigger — perfusion deficits lead to lamellar death, which in turn allows mechanical displacement to catastrophically follow. Thus restoring circulation comes before mechanical correction.
Treatment Protocols: Redden’s Mechanical Strategy
Q: What do his shoes actually do?
Redden’s Four‑Point Trim maximises heel height, frog engagement, and palmar ground contact. He then fits one of his specialized shoes—Ultimate, Drop‑Forge Rail, Four‑Point—each designed to shift GRF palmarly and reduce DDFT tension. The goal: realign P3 mechanically while the lamellar interface recovers ([turn0search0])Redden DVM+1Reddit+1.

Fig 5. The Redden Ultimate shoe showing break-over and heel elevation zones.
Q: How well does this work?
In cases that followed his imaging-guided protocol, Redden has reported realignment success in 70–80% of chronic laminitis cases—a notably higher performance than standard farriery (approximately 50%). Importantly, he avoids nail trauma by using glue or casts where possible.
table 1. Comparisons of treatment outcomes and unintended consequences.
| Mechanism | Redden Reported Success (%) | Foot Trauma Risk | Diagnostic Feedback |
|---|
| Heart‑bar / wedge shoe | Palmar elevation, toe roll | ~50 | Moderate (nails) | Limited |
| Foam pad / impression material | Shock absorption, hoof cushioning | ~30 | Low | Minimal |
| Redden Four‑Point Trim + Shoe | GRF shift, heel loading, break‑over reposition | ~70–80 | Low (glue/cast) | High (via radiographs/venograms) |
| Redden + DDF Tenotomy | Tendon release, derotation | ~80 (with mechanical) | High (surgical) | High |
Surgical Options: Edge Cases Only
Q: When does surgery enter the picture?
Redden is conservative. He may recommend dorsal wall ablation only if the venogram shows perfusion intact below the coffin bone—otherwise it risks leading to sloughing or non-healing. If it’s done, it’s coupled immediately with mechanical shoeing.
Q: What about tenotomy?
Deep digital flexor ligament release is rare in Redden’s practice—but he has recommended it when mechanical therapy fails entirely. Even in external studies, tenotomy is a last resort with survival rates of 59–77%, so its use reflects critical loss of mechanical viability (though Redden insists on immediate orthotic support post-surgery).

Fig 6. A DDFT tenotomy can be performed reliably with a percutaneous cutting thread technique. However, refinement of the technique is required to minimise iatrogenic damage.
Clinical Decision-Making: The Redden Blueprint
His thought process follows a clear sequence:
Take a detailed history, radiographs, and (if needed) video of gait.
Perform a standing venogram to map perfusion.
Classify each case: venogram grade, P3 rotation vs sinking, soft tissue and bone measures, sole thickness, ambulatory status.
Choose treatment pathway: shoe and trim, with or without surgery.
Monitor — weekly x-rays or venograms, adjust mechanical support as growth and perfusion change.
This loop of imaging-guided action provides clarity—and it’s why he offers remote consultations—to ensure accuracy at each phase.
Redden vs Tradition: Why Does It Matter?
Table Suggestion:
Traditional approaches rely on symptom relief, but lack insight into vascular status or alignment trajectory. Redden’s process, while more resource-intensive, offers measurable—and reportedly better—results for chronic, severe laminitis.
The Future: Prosthetics & Custom Manufacturing
Redden and colleagues are developing 3D-scanned hoof-based prosthetic platforms—the next generation of his shoe designs. Tailored manufacturing offers revolutionary potential—to match biomechanics precisely and
 fig 6.ProstheticshavebeenpioneeredbyDr.Redden over the last 25 years and have proved a valuable life saving technique for some. Clearly more research needs to be conducted however modern technology offers hope for many of the most severe cases.
fig 6.ProstheticshavebeenpioneeredbyDr.Redden over the last 25 years and have proved a valuable life saving technique for some. Clearly more research needs to be conducted however modern technology offers hope for many of the most severe cases.
End-of-Article Reflection: What We Learn
When professionals ask: “Is Redden’s approach overkill?”, remember that chronic laminitis lacks universally recognised prognostic metrics—without imaging, we’re guessing. Redden built his method to see what others can’t—and to act only when data supports it.
He requires patience, precision, and advanced imaging—but ultimately offers survival instead of surrender. His work asks: are our treatments based on convenience—or on clarity?
References
Nanric.com (2024) The Tipping Point: How Venograms Make the Difference Between Success and Failure When Treating Laminitis. NANRIC
Redden, R.F. (2001) ‘A Technique for Performing Digital Venography in the Standing Horse’, Equine Veterinary Education, 13(3), pp. 172–178. Redden DVM+2veterinaryevidence.org+2NANRIC+2
Redden, R.F. (2008) ‘Hoof Correction According to Redden in the Chronically Laminitic Horse’, Proceedings, International Laminitis Symposium, Berlin, pp. 194–209. Wikipedia+15veterinaryevidence.org+15NANRIC+15
Redden, R.F. (latest) About – International Equine Podiatry Center. innovativeequinepodiatry.blogspot.com+3Redden DVM+3Redden DVM+3
Rucker, A. et al. (2006) How to Perform the Digital Venogram, AAEP Proceedings, Texas.naturalhorsetrim.com+2veterinaryevidence.org+2NANRIC+2