
A Biomechanical and Therapeutic Review of Equine Laminitis
Two-Part EVA Clog System with Advanced Manufacturing Applications
Author: Mark Caldwell PhD FWCF.
Email: info@hoofflix.com
Keywords: equine laminitis; biomechanics; EVA clog; adhesive farriery; 3D printing; P3 displacement; hoof rehabilitation
Abstract
Equine laminitis is a multifactorial, biomechanically driven disease characterized by inflammation and failure of the dermal-epidermal lamellar interface, leading to displacement of the distal phalanx (P3) and significant lameness. Mechanical forces—ground reaction forces (GRF) and tension from the deep digital flexor tendon (DDFT)—compound lamellar failure, resulting in P3 rotation or sinking. This comprehensive review synthesizes current understanding of etiologies (endocrinopathic, inflammatory, mechanical) and evaluates farriery methods through a SWOT analytical lens. We introduce a modular, two-part glue-on EVA clog system featuring a removable treatment plate and adhesive base, designed to redistribute load, stabilize the hoof capsule, and avoid nail trauma. A case is made for integrating 3D scanning and additive manufacturing to custom-produce clogs optimized for individual hoof mechanics. Future research directions include biomechanical trials, outcome tracking, and wider clinical evaluation.
1. Introduction
Laminitis in horses involves failure of the laminar interface suspending the distal phalanx (P3) within the hoof capsule. While inflammation has long been a focus, accumulating evidence indicates that laminitis is predominantly a biomechanical failure, triggered by metabolic, inflammatory, or structural insults and exacerbated by mechanical load (Mitchell, Fugler & Eades, 2014; Pollitt & Visser, 2010). Radiographic markers such as lamellar zone widening, palmar angle shift, and P3 displacement correlate strongly with clinical severity (Redden, 2003). Catastrophic “sinkers” exhibit vertical droop of P3 with concomitant proximal hoof capsule movement, a pattern consistent with Newtonian prediction of force vectors and tissue yield thresholds (Coffman et al., 1970). Current farriery lacks consistency and often involves invasive shoeing techniques that risk further damage. This work proposes a trauma-free, modular, EVA-based clog system that addresses biomechanical deficits, and examines opportunities for individualised production via 3D printing.
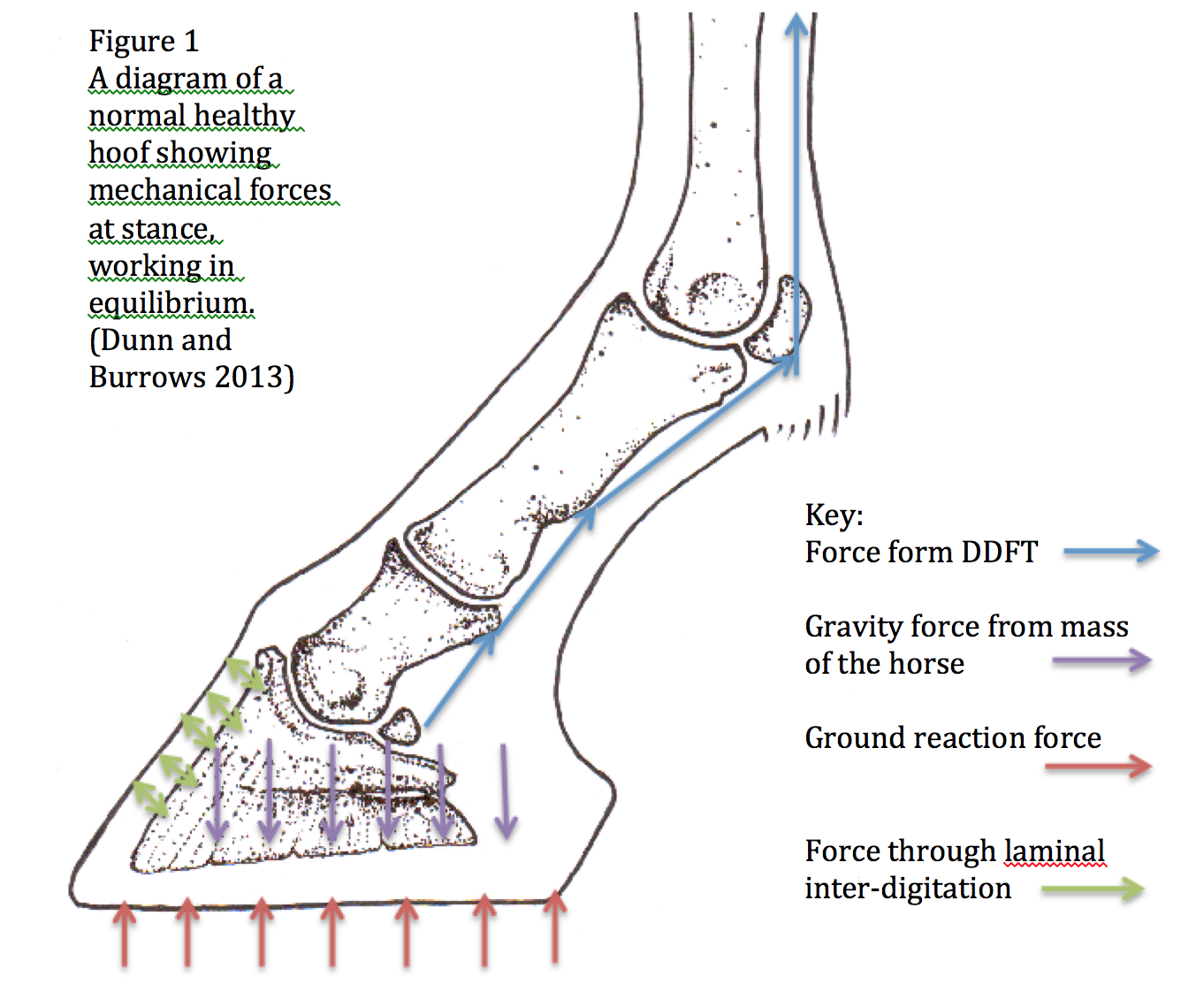
Figure 1. Diagram illustrating biomechanical forces in laminitis: GRF vector, DDFT tension, lamellar interface, and the mechanics of P3 rotation/sinking.
2. Pathophysiology and Etiology
Laminitis originates from systemic triggers that weaken the basement membrane and lamellar suspensory apparatus. Etiologies include endocrinopathy (EMS, PPID), sepsis, carbohydrate overload, and support-limb compromise (Pollitt & Visser, 2010). Once structural integrity is lost, GRF and DDFT forces drive P3 into pathological positions, either rotating dorsally (rotation) or descending vertically through the weakened lamellar bed, manifesting as “sinker” syndrome (Coffman et al., 1970).
Radiographic thresholds inform prognosis and management strategies. Lamellar zone widths over 18 mm, palmar angles exceeding 11°, or P3 rotations over 10–12° are strongly associated with severe outcomes (Redden, 2003; Orsini et al., 2010).
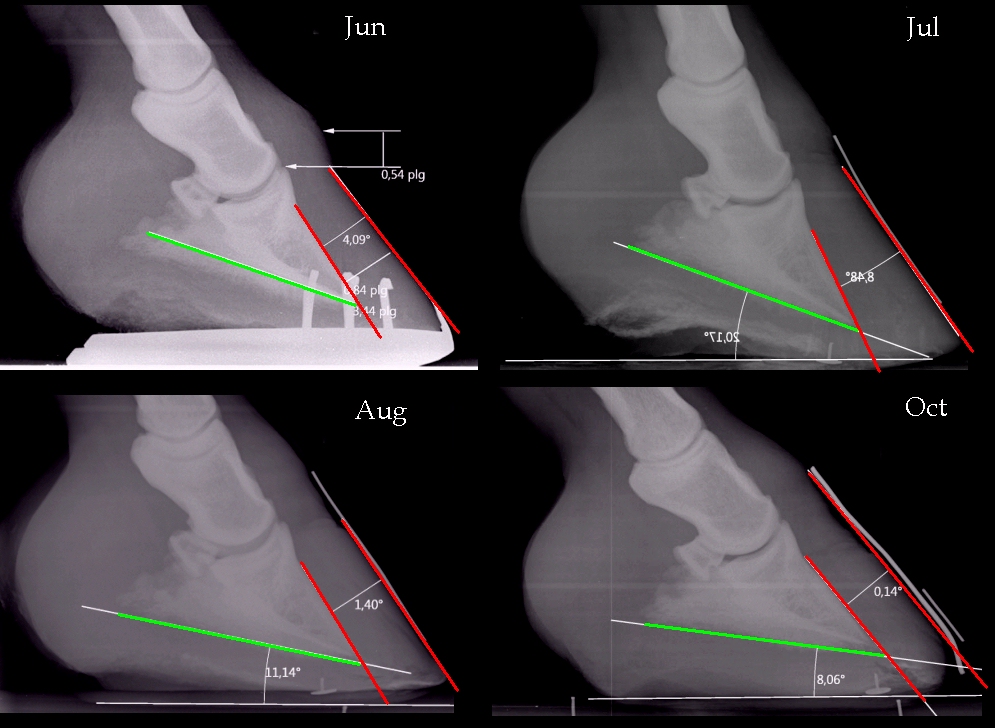
Figure 2. Radiographic series showing progressive stages: (a) healthy hoof; (b) rotation-phase; (c) sinking-phase laminitis. Measurement annotations detail lamellar zone, palmar angle, and P3 alignment (photo credit; The Laminitis Site).
Table 1. Radiographic criteria for laminitis severity
| Parameter | Normal | Pathologic |
|---|---|---|
| Lamellar zone width | 15–17 mm | >18 mm |
| Palmar angle | 3–5° | >11° |
| P3 rotation | <5° | >10–12° |
3. Farriery Approaches and SWOT Analysis
Farriery methods vary from foam pads to heart-bar and wedge shoes. The wooden shoe (or EVA clog) stabilizes the hoof via load redistribution, breakover shift, and heel elevation, often applied non-invasively using screws, glue, or casting tape (O’Grady & Steward, 2009; Equipodiatry, 2025).
SWOT Analysis:
Strengths: Improves palmar support and reduces dorsal loading; modifiable heel angles.
Weaknesses: Inconsistent practitioner skill; lack of robust clinical data.
Opportunities: Custom additive manufacturing; improved scanning and design collaboration.
Threats: Cost barriers; slow adoption in traditional practice.
4. The Modular Two-Part EVA Clog System
This system comprises an adhesive, rigid EVA base contoured to the ground, a deformable EVA foot surface for padding, and a removable treatment plate permitting direct access for dressing or adjustments.
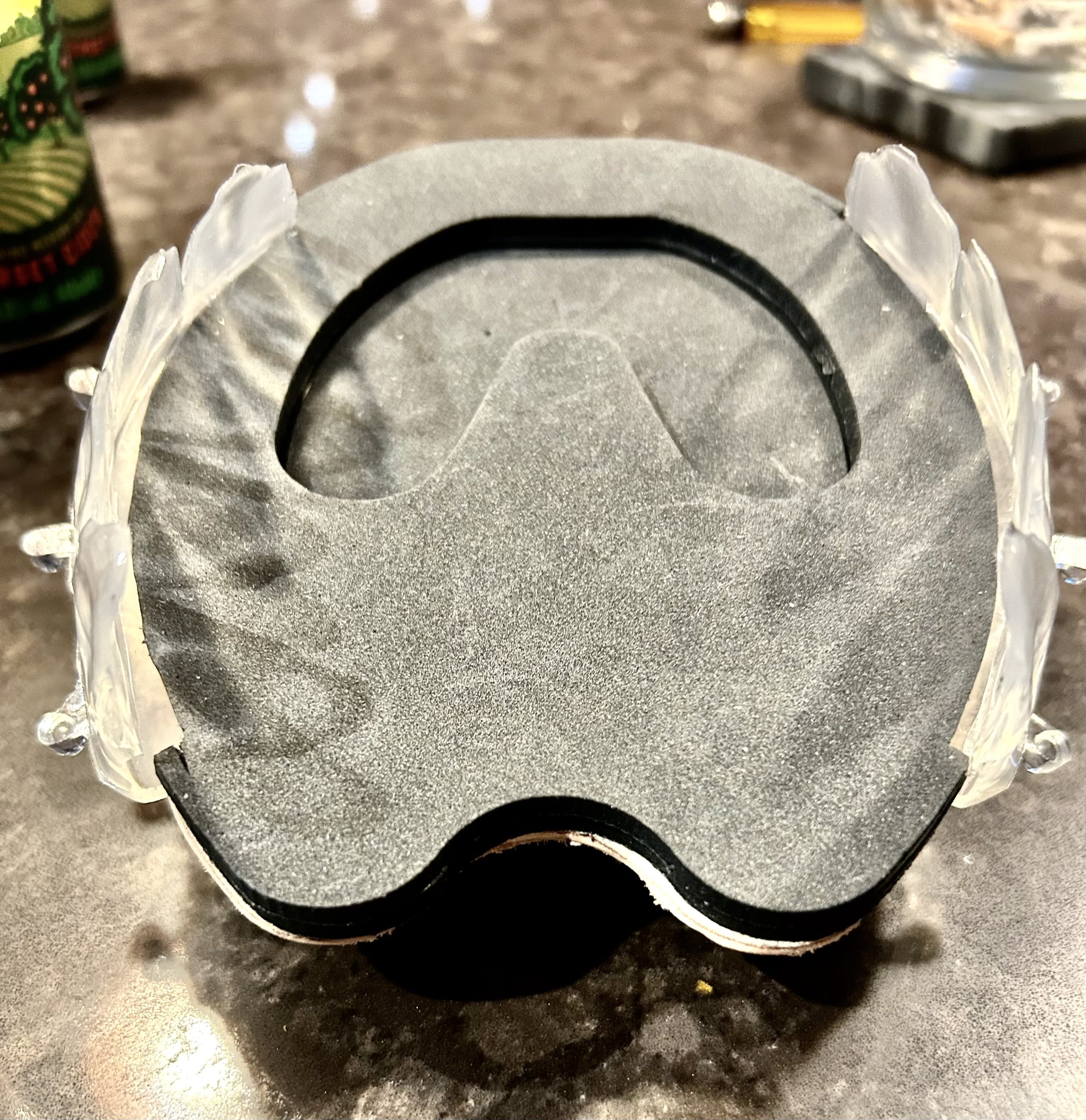


Figure 4. Exploded diagram: 1) ground plate; 2) EVA cushion; 3) removable plate; 4) adhesive interface.
4.1 Application Protocol
Trim hoof per radiographic guidance for optimal palmar angle and base length.
Apply EVA base with non-toxic adhesive.
Attach removable plate for medial hoof access.
Weekly reassessment with radiographs; shoe adjustments made accordingly.
Option to perform 3D scan post-initial stabilization for manufacturing custom clog.
4.2 Mechanistic Benefits
Shifts centre of pressure palmarly, reducing GRF leverage on dorsal lamellae.
Mitigates DDFT tension through controlled heel elevation.
Cushioned EVA distributes pressure across sole and frog.
Modular design facilitates targeted medical intervention.
5. Additive Manufacturing
3D hoof scanning technology captures foot geometry, enabling CAD-design of custom clogs aligned to individual limb biomechanics. Material layering techniques combine rigid and flexible sections, with prototypes successfully trialed in athletic and laminitic equids (TheHorse.com,
6. Alternative Management Methods
Other modalities provide adjunctive support in severe or unresponsive laminitis cases:
6.1 Dorsal Wall Resection
Removing necrotic dorsal wall can relieve pressure. A study of 21 ponies showed improved outcomes in over half treated surgically vs conservative therapy (Pell, 1991).
6.2 Deep Digital Flexor Tenotomy
In refractory laminitis, DDFT tenotomy has produced pasture soundness in up to 77% of cases and 59% survived to two years post-operatively (Eastman et al., 1999; Allen et al., 1986). A newer Brazilian study confirmed repositioning of P3 in 7 chronic cases (Cestari et al., 2022). Tenotomy is best when paired with immediate mechanical stabilization to prevent malalignment (Eastman et al., 1999; AAEP, 2021).
6.3 Cryotherapy
Cooling distal limbs within 48–72 hours of insult reduces lamellar damage and is most efficacious in early phases (Van Eps & Pollitt, 2004).
6.4 Shockwave and Biologics
ESWT and PRP have limited or inconsistent benefits (Seidel et al., 2021). ESWT lacks strong evidence for laminitis, and PRP does not enhance normal hoof growth.
6.5 Acupuncture
Chronic laminitis may respond modestly to acupuncture (OR ~2.3), yet methodological variability limits generalization (Faramarzi et al., 2017).
7. Future Research in Farriery Treatments
Evidence-based farriery requires biomechanical validation and outcome-based clinical data (Weller, 2018).
7.1 Comparative Trials
Randomized studies comparing EVA clog systems to standard shoes, with metrics including lamellar width, palmar angle realignment, and gait parameters.
7.2 Biomechanical Modeling
Finite Element Analysis and in vivo force studies on GRF, breakover timing, and DDFT tension in response to shoing modifications.
7.3 Custom Manufacturing
Clinical trials of 3D printed clogs versus off-the-shelf devices, evaluating fit, function, and hoof-health metrics.
7.4 Prognostic Databases
Multicenter collection of radiographic and clinical data to define validated prognostic indicators (e.g., lamellar measurements, palmar angle, severity index).
8. Discussion
Laminitis requires a flexible treatment matrix based on disease severity, phase, and individual biomechanics. Standard farriery protocols offer symptomatic relief, but iatrogenic damage and inconsistent outcomes persist. Prognostic uncertainty, due to limited large-scale data, complicates management and client communication (Cripps & Eustace, 1999; Orsini et al., 2010).
A modern approach should include:
Acute pain control, cryotherapy, stall rest.
Early mechanical stabilization with EVA clog systems directing GRF support to palmar hoof.
Surgical or wall-resection adjuncts in severe cases.
Custom manufacturing via 3D scanning and printing for individualized load control.
Dynamic reassessment through radiographic and biomechanical monitoring.
The proposed EVA clog model offers a viable, evidence-based bridge across these therapeutic tiers—combining mechanical support, clinical flexibility, and readiness for modern manufacturing scalability.
9. Conclusion
By combining medical, biomechanical, and manufacturing innovation, the two-part EVA clog presents a new standard in customizable, non-invasive laminitis management. Future validation through mechanical analysis and clinical outcome studies is both feasible and necessary to advance hoof health care.
References
Allen, D.A. et al. (1986) ‘Mid-metacarpal deep digital flexor tenotomy in chronic laminitis’, Vet Surgery, 15(4), pp. 292–298.americanfarriers.com+9equipodiatry.com+9thelaminitissite.org+9avmajournals.avma.orgthelaminitissite.orgamericanfarriers.comequipodiatry.comavmajournals.avma.org+5pubmed.ncbi.nlm.nih.gov+5ivis.org+5en.wikipedia.org+1en.wikipedia.org+1
Cestari, H. et al. (2022) ‘DDF tenotomy & DP realignment in chronic laminitis’, Research Society and Development, 11(13), e313111335298. researchgate.net
Coffman, J.R. et al. (1970) ‘Vertical displacement in laminitis’, Am J Vet Res, 31, pp. 221–225.
Cripps, P.J. & Eustace, R.A. (1999) ‘Laminitis prognosis’, Equine Vet J, 31(5), pp. 433–442.
Eastman, T.G. et al. (1999) ‘DDF tenotomy outcomes’, J Am Vet Med Assoc, 214(4), pp. 517–519.
Equipodiatry. (2025) ‘Farriery options in laminitis’, Equipodiatry.com.
Faramarzi, B. et al. (2017) ‘Acupuncture in laminitis’, Can Vet J, 58(8), pp. 823–827.